Perioperative cutaneous complications in an elderly patient due to inappropriate use of a forced-air warming device and underbody blanket: a case report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Inje University Busan Paik Hospital, Busan, Korea
- KMID: 2549502
- DOI: http://doi.org/10.7180/kmj.23.136
Abstract
- Forced-air warming is commonly utilized to prevent perioperative hypothermia. Underbody warming blankets are often employed to secure a larger area for patient warming. While forced-air warming systems are generally regarded as safe, improper usage poses a risk of cutaneous complications. Additionally, the influence of underbody blankets on cutaneous complications remains uncertain. We present a case of cutaneous complications resulting from the improper utilization of a forced-air warming device and an underbody blanket. A 79-year-old man presented to the hospital for robotic proctectomy under general anesthesia. The surgery lasted for 7 hours, and the forced-air warming device with underbody blanket operated continuously for 5 hours intraoperatively. The surgery was completed without any incidents. However, first-degree burns on the patient’s back, along with superficial decubitus ulcers on his right scapula, were observed after surgery. To prevent cutaneous complications, clinicians must adhere to the manufacturer's guidelines when utilizing a forced-air warming system. Compared to overbody blankets, underbody blankets have limitations in monitoring cutaneous responses. Ensuring patient safety requires selecting an appropriate blanket for scheduled operations.
Keyword
Figure
-
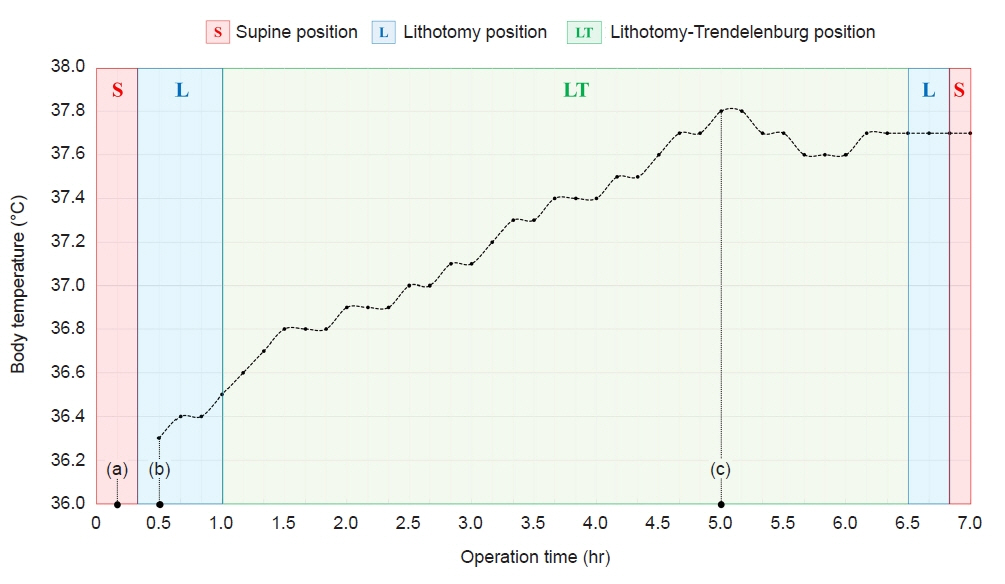
Fig. 1. Changes in body temperature and surgical position. (a) Start of induction of general anesthesia. (b) Start measuring body temperature. (c) Turning off the forced-air warming system. The changes in the patient's position during surgery are differentiated by boxes of different colors.

Fig. 2. Lithotomy-Trendelenburg position. Bilateral shoulder supports (black arrowheads) were used so that the patient would not slip from the bed intraoperatively.

Fig. 3. Skin erosions on the right scapula. The areas of erosion measured 10×5 and 5×8 cm. The image has been altered to obscure any personal identifying information of the patient.

Fig. 4. Reddish linear skin lesions around the shoulder. The image has been altered to obscure any personal identifying information of the patient.
Reference
-
References
1. Simegn GD, Bayable SD, Fetene MB. Prevention and management of perioperative hypothermia in adult elective surgical patients: a systematic review. Ann Med Surg (Lond). 2021; 72:103059.2. Sumida H, Sugino S, Kuratani N, Konno D, Hasegawa JI, Yamauchi M. Effect of forced-air warming by an underbody blanket on end-of-surgery hypothermia: a propensity score-matched analysis of 5063 patients. BMC Anesthesiol. 2019; 19:50.3. Ackermann W, Fan Q, Parekh AJ, Stoicea N, Ryan J, Bergese SD. Forced-air warming and resistive heating devices: updated perspectives on safety and surgical site infections. Front Surg. 2018; 5:64.4. Wu X. The safe and efficient use of forced-air warming systems. AORN J. 2013; 97:302–8.5. Im SI. How to write case reports in medicine. Kosin Med J. 2022; 37:102–6.6. Yoo JH, Ok SY, Kim SH, Chung JW, Park SY, Kim MG, et al. Comparison of upper and lower body forced air blanket to prevent perioperative hypothermia in patients who underwent spinal surgery in prone position: a randomized controlled trial. Korean J Anesthesiol. 2022; 75:37–46.7. Brauer A, Quintel M. Forced-air warming: technology, physical background and practical aspects. Curr Opin Anaesthesiol. 2009; 22:769–74.8. Sikka RS, Prielipp RC. Forced air warming devices in orthopaedics: a focused review of the literature. J Bone Joint Surg Am. 2014; 96:e200.9. Zaidi SRH, Sharma S. Pressure ulcer. StatPearls [Internet]. StatPearls Publishing; 2023 [cited 2023 Aug 28]. http://www.ncbi.nlm.nih.gov/books/NBK553107/.10. Landsberg L, Young JB, Leonard WR, Linsenmeier RA, Turek FW. Do the obese have lower body temperatures? A new look at a forgotten variable in energy balance. Trans Am Clin Climatol Assoc. 2009; 120:287–95.11. Chung K, Lee S, Oh SC, Choi J, Cho HS. Thermal burn injury associated with a forced-air warming device. Korean J Anesthesiol. 2012; 62:391–2.12. Brauer A, Perl T, Heise D, Quintel M, Seipelt R. Intraoperative full-thickness pressure ulcer in a patient after transapical aortic valve replacement using a novel underbody forced-air warming blanket. J Clin Anesth. 2010; 22:573–4.13. National Institute for Health and Care Excellence (NICE). Hypothermia: prevention and management in adults having surgery [Internet]. NICE; 2016 [cited 2023 Aug 29]. http://www.ncbi.nlm.nih.gov/books/NBK554181/.14. Wang J, Fang P, Sun G, Li M. Effect of active forced air warming during the first hour after anesthesia induction and intraoperation avoids hypothermia in elderly patients. BMC Anesthesiol. 2022; 22:40.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of upper and lower body forced air blanket to prevent perioperative hypothermia in patients who underwent spinal surgery in prone position: a randomized controlled trial
- Effects of Forced-Air Warming Therapy on Anxiety, Pain, and Body Temperature of Patients under Local Anesthesia during Surgery: A Quasi-Experimental Study
- The Effects of Active Warming on Pain, Temperature, and Thermal Discomfort in Postoperative Patients after General Anesthesia for Abdominal Surgery
- Effect of short-term prewarming on body temperature in arthroscopic shoulder surgery
- The efficacy of warming blanket on reducing intraoperative hypothermia in patients undergoing transurethral resection of bladder tumor under general anesthesia
