Squamous cell carcinoma of lower lip: the results of wide V-shaped resection
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Seoul National University, Seoul, Korea
- 2Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea
- KMID: 2547574
- DOI: http://doi.org/10.5125/jkaoms.2023.49.5.292
Abstract
- Generally, if the size of a lip cancer defect exceeds 30% of the lower lip, a local flap or free flap is recommended. However, defects up to 50% of the lower lip in size have been reconstructed successfully by primary closure without a local flap or free flap. In one case, an 80-year-old male farmer who had smoked for more than 50 years presented with squamous cell carcinoma of the lower lip and underwent mass resection and supraomohyoid neck dissection. The defect accounted for almost 2/3 of the lower lip and was repaired by primary closure with V-shaped resection. Biopsy results confirmed pT2N0cM0 stage II disease with clear margins. In another case, a 68-year-old male also presented with squamous cell carcinoma of the lower lip and underwent mass resection. The defect accounted for about half the size of the lower lip but was repaired by primary closure with V-shaped resection. Both patients experienced no discomfort while eating or speaking and were satisfied with the cosmetic and functional outcomes with no evidence of recurrence. Thus, direct closure can be considered even in large lower lip cancers.
Figure
-

Fig. 1 Preoperative clinical photo and enhanced computed tomography (CT) view. A tumor mass approximately 2.5 cm in diameter crosses the wet-dry border of the oral cavity. A, B. Clinical photos. C. CT axial view. D. Magnetic resonance imaging axial view.
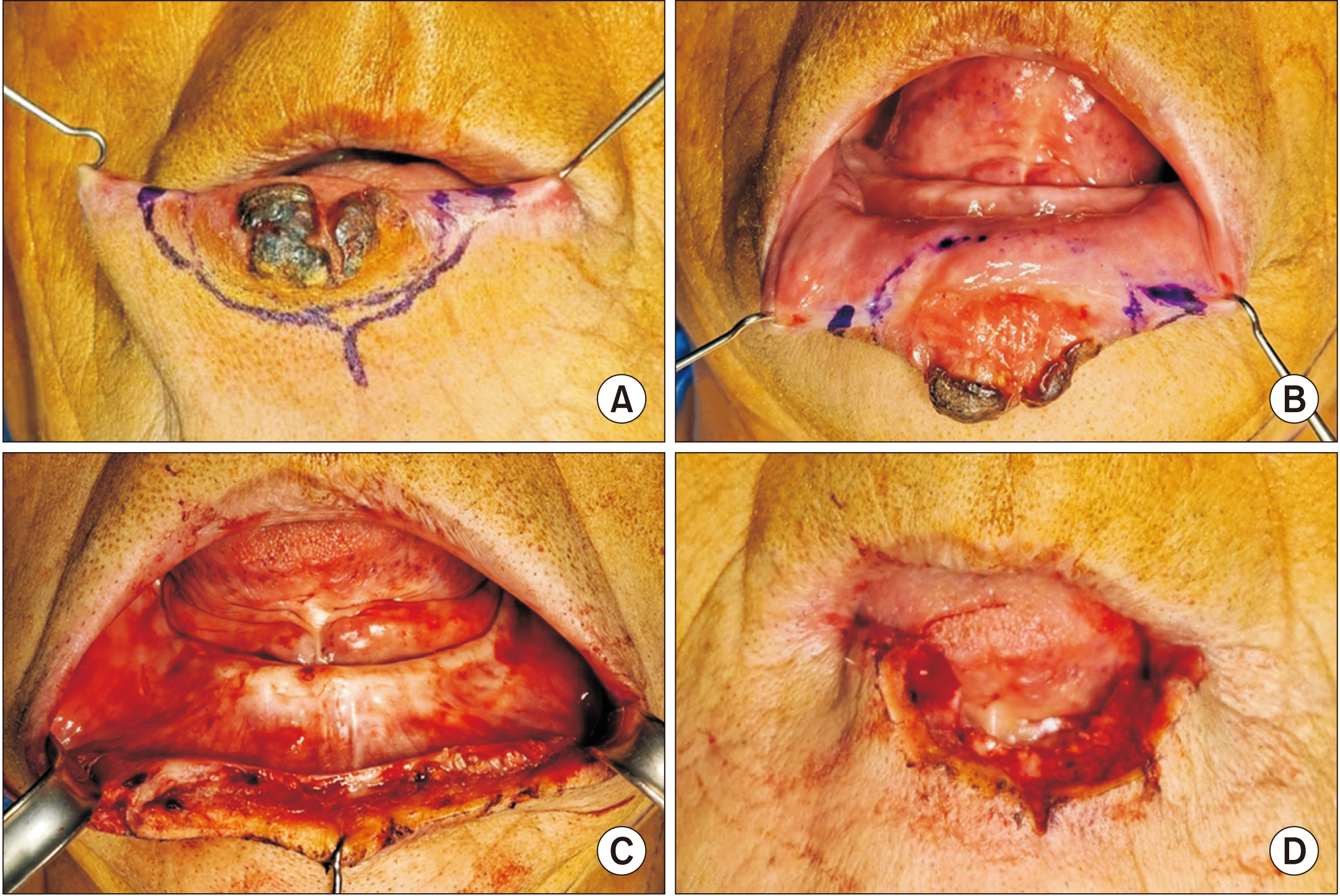
Fig. 2 Intraoperative clinical photo. The mass was excised with a safety margin using a V-shaped incision. A, B. Clinical images before operation. C, D. Clinical images after operation.

Fig. 3 Clinical photo three days postoperative. The defect was restored with direct closure.
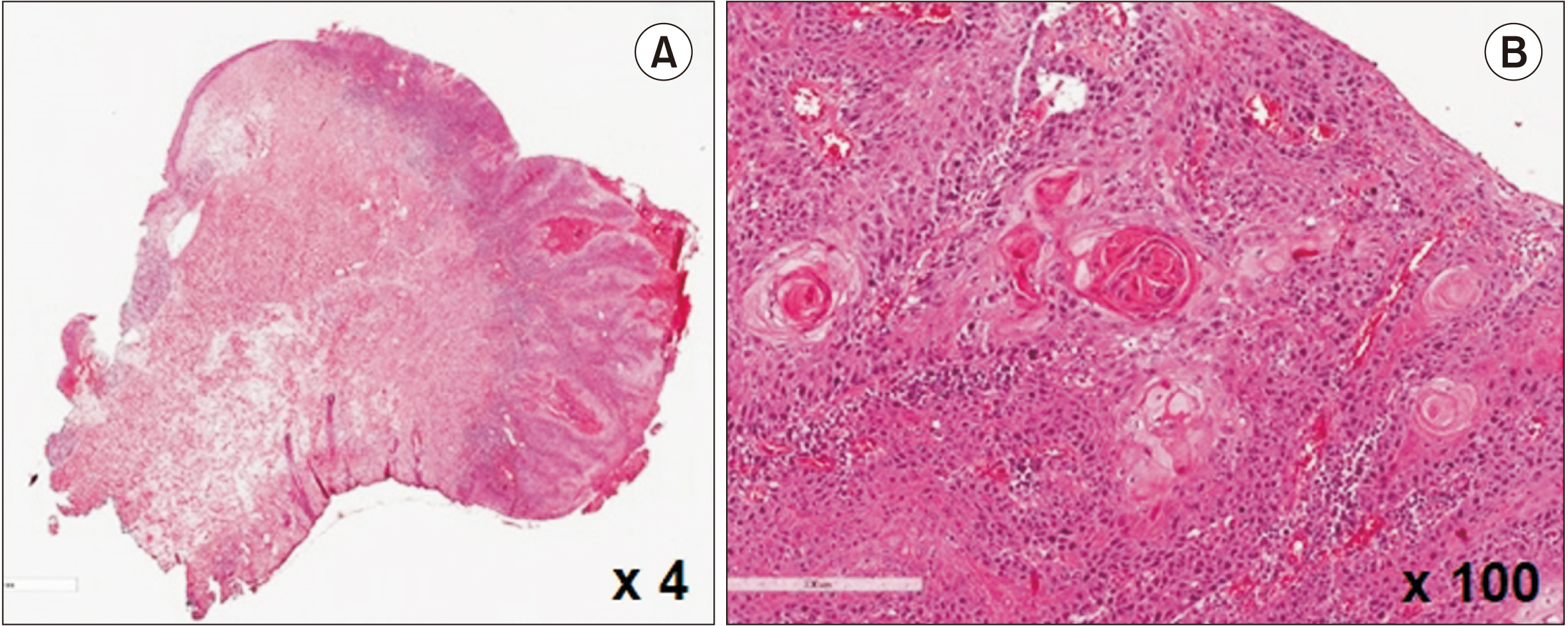
Fig. 4 Histopathologic view of the main mass. Keratin pearls can be identified in the histopathologic image (H&E staining, A: ×4, B: ×100).
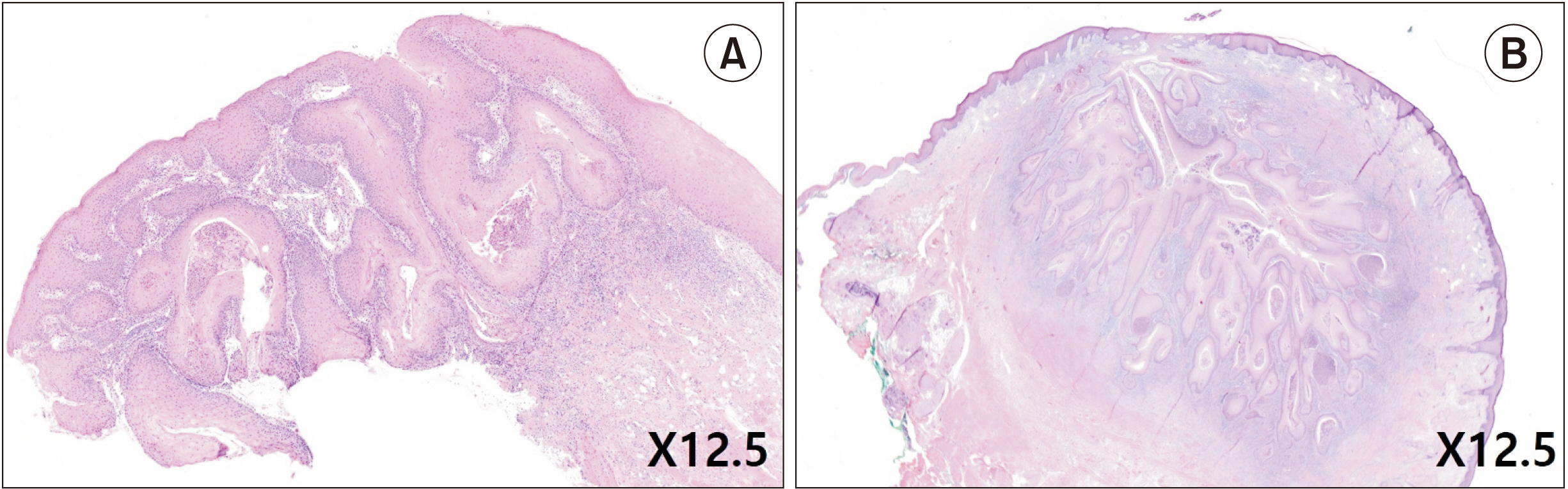
Fig. 5 The H&E stained histopathologic specimen from the incisional biopsy performed on the first visit (A) and the main mass (B) in Case 2. A. At first the lesion was diagnosed as dysplasia due to lack of tumor invasion of the basement membrane. B. The main mass from the surgery was diagnosed as squamous cell carcinoma (H&E staining, A: ×12.5, B: ×12.5).

Fig. 6 Preoperative clinical photograph of the lower lip tumor in Case 2.
Reference
-
References
1. Ozturk K, Gode S, Erdogan U, Akyildiz S, Apaydin F. 2015; Squamous cell carcinoma of the lip: survival analysis with long-term follow-up. Eur Arch Otorhinolaryngol. 272:3545–50. https://doi.org/10.1007/s00405-014-3415-6. DOI: 10.1007/s00405-014-3415-6. PMID: 25467011.
Article2. Bota JP, Lyons AB, Carroll BT. 2017; Squamous cell carcinoma of the lip-a review of squamous cell carcinogenesis of the mucosal and cutaneous junction. Dermatol Surg. 43:494–506. https://doi.org/10.1097/dss.0000000000001020. DOI: 10.1097/DSS.0000000000001020. PMID: 28157733.
Article3. Matin MB, Dillon J. 2014; Lip reconstruction. Oral Maxillofac Surg Clin North Am. 26:335–57. https://doi.org/10.1016/j.coms.2014.05.013. DOI: 10.1016/j.coms.2014.05.013. PMID: 25086695.
Article4. Boukovalas S, Boson AL, Hays JP, Malone CH, Cole EL, Wagner RF. 2017; A systematic review of lower lip anatomy, mechanics of local flaps, and special considerations for lower lip reconstruction. J Drugs Dermatol. 16:1254–61. PMID: 29240861.5. Malard O, Corre P, Jégoux F, Durand N, Dréno B, Beauvillain C, et al. 2010; Surgical repair of labial defect. Eur Ann Otorhinolaryngol Head Neck Dis. 127:49–62. https://doi.org/10.1016/j.anorl.2010.04.001. DOI: 10.1016/j.anorl.2010.04.001. PMID: 20822758.
Article6. Krunic AL, Weitzul S, Taylor RS. 2005; Advanced reconstructive techniques for the lip and perioral area. Dermatol Clin. 23:43–53. v–vi. https://doi.org/10.1016/j.det.2004.08.009. DOI: 10.1016/j.det.2004.08.009. PMID: 15620618.
Article7. Baker SR. 2007. Local flaps in facial reconstruction. 2nd ed:Mosby;DOI: 10.1016/B978-0-323-03684-9.50023-2.8. Neligan PC. 2013. Plastic surgery. 3rd ed:Elsevier;DOI: 10.1016/j.det.2004.08.009.9. McCarn KE, Park SS. 2005; Lip reconstruction. Facial Plast Surg Clin North Am. 13:301–14. viihttps://doi.org/10.1016/j.fsc.2004.11.005. DOI: 10.1016/j.fsc.2004.11.005. PMID: 15817408.
Article10. Anvar BA, Evans BCD, Evans GRD. 2007; Lip reconstruction. Plast Reconstr Surg. 120:57e–64e. https://doi.org/10.1097/01.prs.0000278056.41753.ce. DOI: 10.1097/01.prs.0000278056.41753.ce. PMID: 17805106. PMCID: PMC10484365.
Article11. Demirdover C, Vayvada H, Ozturk FA, Yazgan HS, Karaca C. 2019; A new modification of fan flap for large lower lip defects. Scand J Surg. 108:172–7. https://doi.org/10.1177/1457496918798211. DOI: 10.1177/1457496918798211. PMID: 30178718.
Article12. Sanniec KJ, Carboy JA, Thornton JF. 2018; Simplifying lip reconstruction: an algorithmic approach. Semin Plast Surg. 32:69–74. https://doi.org/10.1055/s-0038-1645882. DOI: 10.1055/s-0038-1645882. PMID: 29765270. PMCID: PMC5951711.
Article13. Soliman S, Hatef DA, Hollier LH Jr, Thornton JF. 2011; The rationale for direct linear closure of facial Mohs' defects. Plast Reconstr Surg. 127:142–9. https://doi.org/10.1097/prs.0b013e3181f95978. DOI: 10.1097/PRS.0b013e3181f95978. PMID: 21200208.
Article14. Harris L, Higgins K, Enepekides D. 2012; Local flap reconstruction of acquired lip defects. Curr Opin Otolaryngol Head Neck Surg. 20:254–61. https://doi.org/10.1097/moo.0b013e3283557dcf. DOI: 10.1097/MOO.0b013e3283557dcf. PMID: 22894993.
Article15. Park CH, Kwon TK, Hong SJ, Chu HR. 2008; Reconstruction after resection of lower lip squamous cell carcinoma. Korean J Otorhinolaryngol Head Neck Surg. 51:471–6.16. Ishii LE, Byrne PJ. 2009; Lip reconstruction. Facial Plast Surg Clin North Am. 17:445–53. https://doi.org/10.1016/j.fsc.2009.05.007. DOI: 10.1016/j.fsc.2009.05.007. PMID: 19698922.
Article17. Jeong DM, Shin YJ, Lee NR, Lim HK, Choung HW, Pang KM, et al. 2017; Maximal strength and endurance scores of the tongue, lip, and cheek in healthy, normal Koreans. J Korean Assoc Oral Maxillofac Surg. 43:221–8. https://doi.org/10.5125/jkaoms.2017.43.4.221. DOI: 10.5125/jkaoms.2017.43.4.221. PMID: 28875136. PMCID: PMC5583196.
Article18. Lupu M, Caruntu A, Caruntu C, Boda D, Moraru L, Voiculescu V, et al. 2018; Non-invasive imaging of actinic cheilitis and squamous cell carcinoma of the lip. Mol Clin Oncol. 8:640–6. https://doi.org/10.3892/mco.2018.1599. DOI: 10.3892/mco.2018.1599. PMID: 29725529. PMCID: PMC5920479.
Article19. Elmas ÖF, Metin MS, Kilitçi A. 2019; Dermoscopic features of lower lip squamous cell carcinoma: a descriptive study. Indian Dermatol Online J. 10:536–41. https://doi.org/10.4103/idoj.idoj_435_18. DOI: 10.4103/idoj.IDOJ_435_18. PMID: 31544072. PMCID: PMC6743386.
Article20. Wood NH, Khammissa R, Meyerov R, Lemmer J, Feller L. 2011; Actinic cheilitis: a case report and a review of the literature. Eur J Dent. 5:101–6. DOI: 10.1055/s-0039-1698864. PMID: 21228959. PMCID: PMC3019754.
Article21. Vieira RA, Minicucci EM, Marques ME, Marques SA. 2012; Actinic cheilitis and squamous cell carcinoma of the lip: clinical, histopathological and immunogenetic aspects. An Bras Dermatol. 87:105–14. https://doi.org/10.1590/s0365-05962012000100013. DOI: 10.1590/S0365-05962012000100013. PMID: 22481658.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of squamous Cell Carcinoma Arising from an Actinic Cheilitis and Its Surgical Treatment
- Large Lower Lip Defect Reconstruction Using a Karapandzic Flap: A Case Report and Literature Review
- Squamous Cell Carcinoma Mimicking Herpes Simplex on the Lip
- Reconstruction of a large lower lip defect using a combination of Abbe and staircase flaps: a case report
- Two cases of aquamous cell carcinoma of the lower lip treated with liquid nitrogen
