Differential diagnosis for unusually dilated coronary sinus and right coronary artery incidentally found on echocardiography
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea
- 2Division of Physiology, Department of Biomedical Laboratory, Daegu Health College, Daegu, Korea
- KMID: 2547375
- DOI: http://doi.org/10.12701/jyms.2023.00906
Figure
-
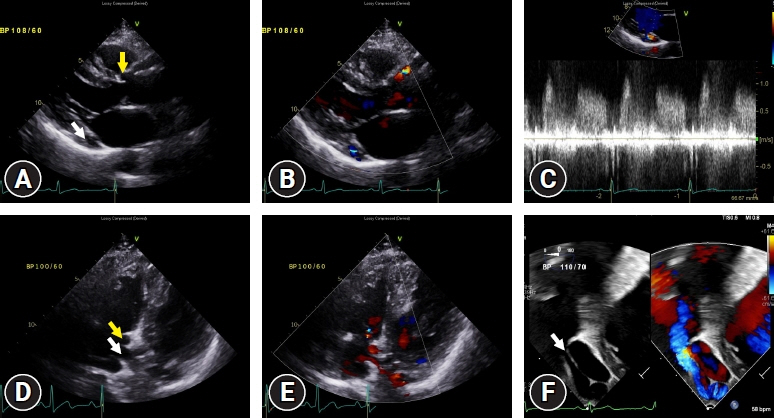
Fig. 1. Transthoracic echocardiography (TTE), parasternal long-axis view showing (A) dilated coronary sinus (CS; white arrow) and right coronary artery (RCA; yellow arrow), (B) aliasing signal at the CS on color Doppler imaging, and (C) continuous flow on pulse-wave Doppler imaging. TTE, subcostal view showing (D) the dilated CS ostium (white arrow) and RCA (yellow arrow), and (E) blood flow from the CS ostium to the right atrium on color Doppler imaging. (F) Turbulent blood flow from the CS ostium (white arrow) was observed by transesophageal echocardiography.
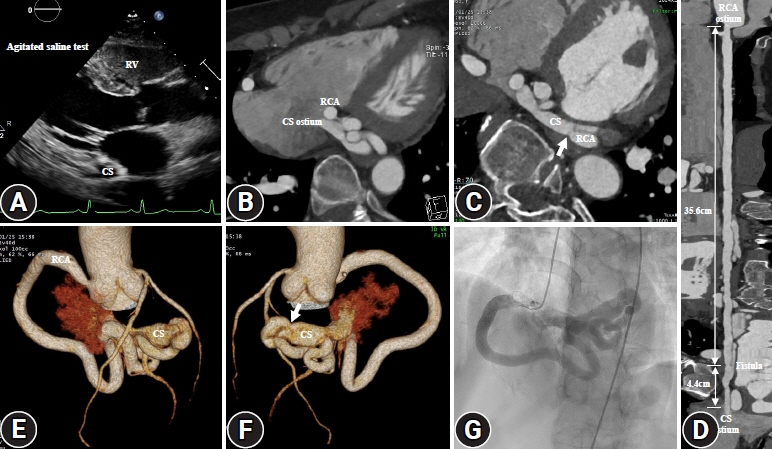
Fig. 2. Transthoracic echocardiography (TTE), parasternal long-axis view showing (A) immediate opacification of the right ventricle (RV), not of the coronary sinus (CS), after injection of agitated saline into a left arm. Cardiac computed tomography (CT), axial imaging, and three-dimensional volume-rendering imaging presenting (B–F) dilated right coronary artery (RCA), fistula (white arrow), and dilated CS. Cardiac CT, multiplanar reformatting imaging presenting (D) the overall course of huge RCA with fistula to the CS. Coronary angiography presenting (G) dilated, tortuous RCA drained to the right atrium.
Reference
-
References
1. Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022; 43:3618–731.
Article2. Goyal SK, Punnam SR, Verma G, Ruberg FL. Persistent left superior vena cava: a case report and review of literature. Cardiovasc Ultrasound. 2008; 6:50.
Article3. Abdel Razek AA, Al-Marsafawy H, Elmansy M, El-Latif MA, Sobh D. Computed tomography angiography and magnetic resonance angiography of congenital anomalies of pulmonary veins. J Comput Assist Tomogr. 2019; 43:399–405.
Article4. Kawsara A, Núñez Gil IJ, Alqahtani F, Moreland J, Rihal CS, Alkhouli M. Management of coronary artery aneurysms. JACC Cardiovasc Interv. 2018; 11:1211–23.5. Pham V, Hemptinne Q, Grinda JM, Duboc D, Varenne O, Picard F. Giant coronary aneurysms, from diagnosis to treatment: a literature review. Arch Cardiovasc Dis. 2020; 113:59–69.
Article6. Abou Sherif S, Ozden Tok O, Taşköylü Ö, Goktekin O, Kilic ID. Coronary artery aneurysms: a review of the epidemiology, pathophysiology, diagnosis, and treatment. Front Cardiovasc Med. 2017; 4:24.
Article7. Gordon JB, Kahn AM, Burns JC. When children with Kawasaki disease grow up: myocardial and vascular complications in adulthood. J Am Coll Cardiol. 2009; 54:1911–20.8. Thangathurai J, Kalashnikova M, Takahashi M, Shinbane JS. Coronary artery aneurysm in Kawasaki disease: coronary CT angiography through the lens of pathophysiology and differential diagnosis. Radiol Cardiothorac Imaging. 2021; 3:e200550.
Article9. Al-Hijji M, El Sabbagh A, El Hajj S, AlKhouli M, El Sabawi B, Cabalka A, et al. Coronary artery fistulas: indications, techniques, outcomes, and complications of transcatheter fistula closure. JACC Cardiovasc Interv. 2021; 14:1393–406.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Rare Combination of the Left Circumflex Coronary Artery Fistula Connecting a Dilated Coronary Sinus with Persistent Left Superior Vena Cava and Multiple Arteriovenous Fistulae
- Two Cases of Anomalous Origin of Coronary Artery
- A Case of Double Right Coronary Artery with Arteriovenous Fisula
- Direct Visualization of Coronary Artery and Flow using Transthoracic Doppler Echocardiography
- Anomalous Origin of the Left Circumflex Coronary Artery: A Report of 2 Cases and Echocardiographic Features
