Awake craniotomy removal of a corticospinal tract developmental venous anomaly hemorrhage: A case report
- Affiliations
-
- 1Department of Neurosurgery, Hospital Privado de Rosario - Grupo Gamma, Rosario, Santa Fe, Argentina
- 2Department of Radiology, Hospital Privado de Rosario - Grupo Gamma, Rosario, Santa Fe, Argentina
- 3Department of Neurophysiology, Hospital Privado de Rosario - Grupo Gamma, Rosario, Santa Fe, Argentina
- KMID: 2546169
- DOI: http://doi.org/10.7461/jcen.2023.E2022.03.004
Abstract
- Developmental venous anomalies (DVAs) are composed of mature venous vessels that lack malformed or neoplastic elements. Although the hemorrhage risk is considered negligible, some patients may have neurological symptoms attributable to acute infarction or intracranial hemorrhage secondary to thrombosis, in the absence of a coexisting cavernous malformation. We report the case of a 42-year-old patient who presented with acute left-hand paresis secondary to a subcortical hemorrhage. This bleeding originated from a DVA in the corticospinal tract area and was surgically drained through an awake craniotomy. To accomplish this, we used a trans-precentral sulcus approach. After the complete removal of the coagulum, small venous channels appeared, which were coagulated. No associated cavernoma was found. Although the main DVA trunk was left patent, no signs of ischemia or venous infarction were observed after coagulating the small venous channels found inside the hematoma cavity. Two weeks after the procedure, the patient’s hand function improved, and he was able to resume desktop work. DVA-associated hemorrhage within the cortico-spinal tract could be safely removed with modern awake mapping techniques. This technique allowed the patient to rapidly improve his hand function.
Keyword
Figure
-
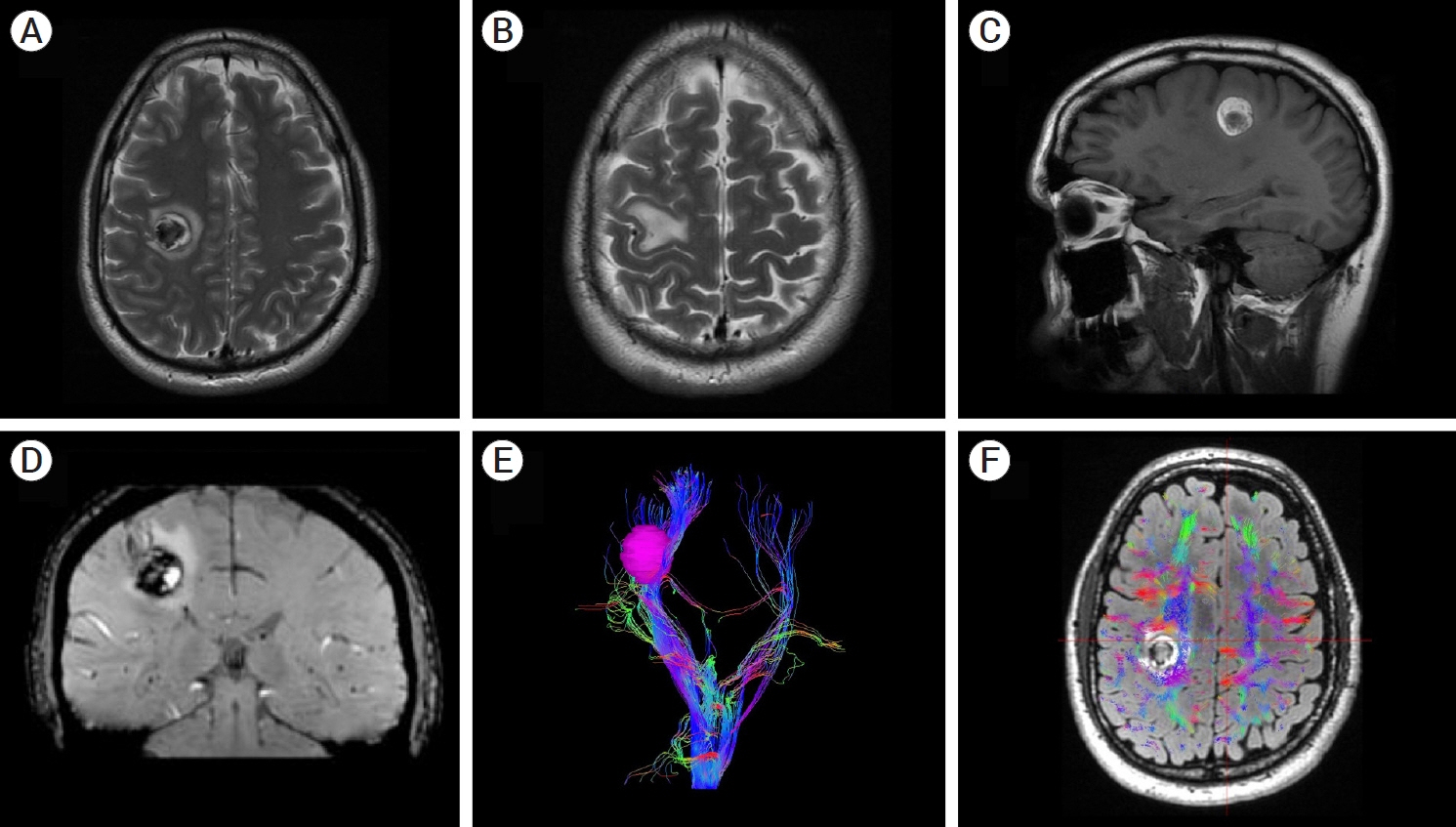
Fig. 1. (A) Axial T2-weighted magnetic resonance imaging (MRI) revealing a 4-cc hypointense lesion. An irregular hyperintense perilesional rim was observed. This lesion was located subcortically, within the corticospinal tract. (B) Axial T2-weighted MRI showing edema at the level of the hand knob. (C) Sagittal non-contrast T1-weighted MRI revealing a hyperintense mass. (D) Coronal SWI-weighted MRI. A developmental venous anomaly is visualized adjacent to the hemorrhage. (E and F) MRI tractography of the corticospinal tract. Note that the hand fibers were spread out by the hemorrhage.
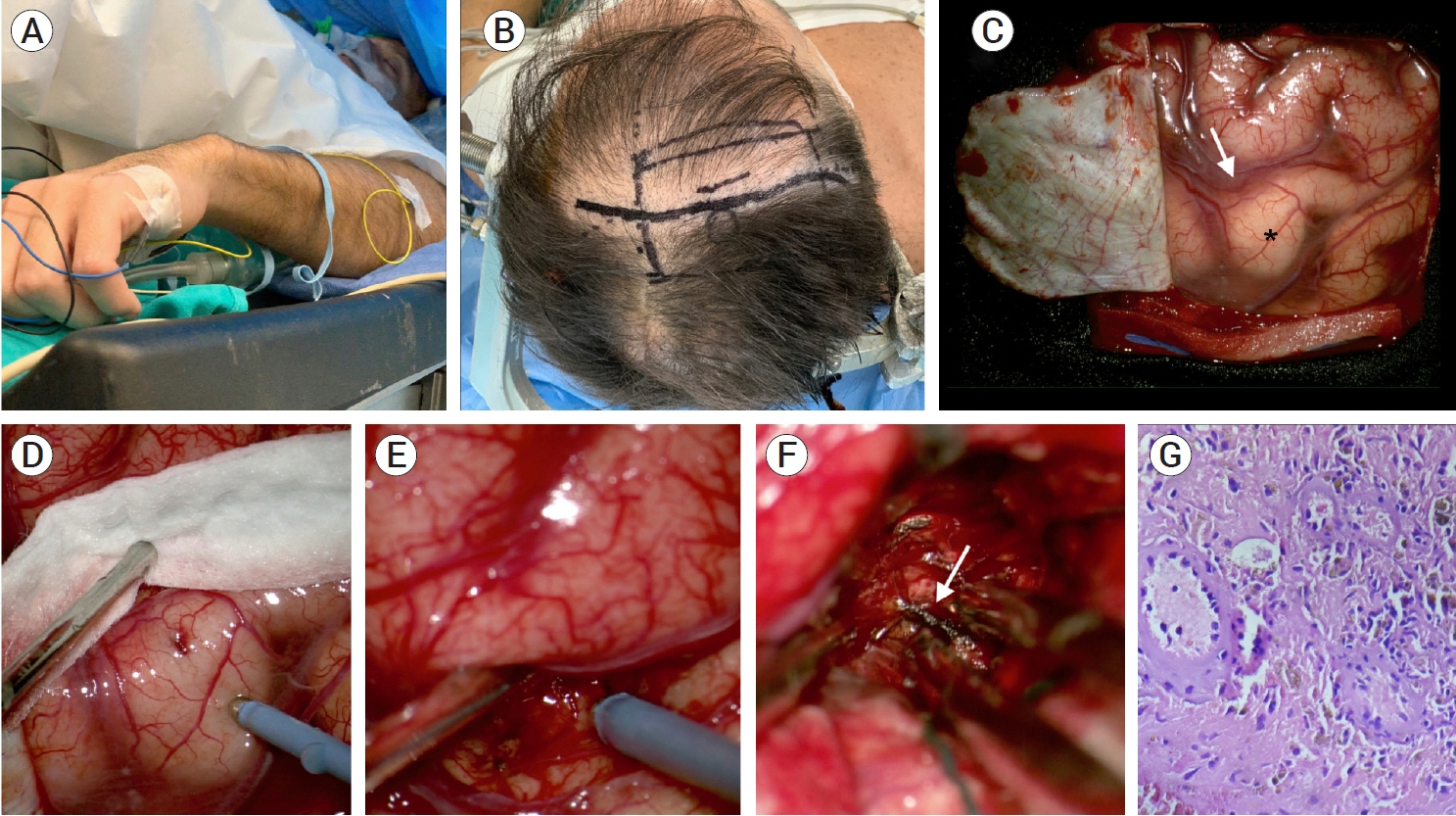
Fig. 2. The patient was operated on awake. (A) Initial step with a nasal cannula. EMG electrodes were placed in his upper and lower extremities. (B) Intraoperative photograph showing the planned craniotomy. A right lazy S incision and frontoparietal craniotomy were performed. (C) Microscopic photograph showing the initial cortical exposure. Note the hand knob (black star) and precentral sulcus (white arrow). (D and E) High-frequency monopolar cortical mapping of the precentral gyrus and sulcus. (F) Exposure of the hemorrhage after opening the precentral sulcus. Several venous channels (white arrow) were found and thoroughly coagulated within the hematoma. No cavernous malformation was found within or adjacent to the hematoma cavity. (G) On hematoxylin and eosin sections, there are small to medium-sized blood vessels and macrophages containing hemosiderin pigment (40×).

Fig. 3. (A) Eight-month axial T2-weighted magnetic resonance imaging (MRI) showing complete resolution of the hemorrhage. (B) Axial T2-weighted MRI at the level of the hand knob. Note mild atrophy of this cortical area. (C and D) MRI tractography of the corticospinal tract. Note the proximity of the resection cavity (white arrow) with this structure. (E) Coronal T1-weighted contrast-enhanced MRI. The main developmental venous anomaly remains patent (white arrow).
Reference
-
1. Barrenechea IJ, Rojas H, Nicola M, Marquez L, Herrera R, Van Isseldyk F. A novel temporary cranial fixation device for awake cranial surgery: technical report of 14 cases. Surg Neurol Int. 2020; Jan. 11:12.2. Frigeri T, Paglioli E, de Oliveira E, Rhoton AL Jr. Microsurgical anatomy of the central lobe. J Neurosurg. 2015; Mar. 122(3):483–98.3. Garner TB, Del Curling O Jr, Kelly DL Jr, Laster DW. The natural history of intracranial venous angiomas. J Neurosurg. 1991; Nov. 75(5):715–22.4. Gempt J, Krieg SM, Hüttinger S, Buchmann N, Ryang YM, Shiban E, et al. Postoperative ischemic changes after glioma resection identified by diffusion-weighted magnetic resonance imaging and their association with intraoperative motor evoked potentials. J Neurosurg. 2013; Oct. 119(4):829–36.5. Hill BD, Barkemeyer CA, Jones GN, Santa Maria MP, Minor KS, Browndyke JN. Validation of the coin rotation test: a simple, inexpensive, and convenient screening tool for impaired psychomotor processing speed. Neurologist. 2010; 16(4):249–53.6. Lasjaunias P, Burrows P, Planet C. Developmental venous anomalies (DVA): the so-called venous angioma. Neurosurg Rev. 1986; Sep. 9(3):233–42.7. McLaughlin MR, Kondziolka D, Flickinger JC, Lunsford S, Lunsford LD. The prospective natural history of cerebral venous malformations. Neurosurgery. 1998; Aug. 43(2):195–200. discussion 200-1.8. Naff NJ, Wemmer J, Hoenig-Rigamonti K, Rigamonti DR. A longitudinal study of patients with venous malformations: documentation of a negligible hemorrhage risk and benign natural history. Neurology. 1998; Jun. 50(6):1709–14.9. Rabinov JD. Diagnostic imaging of angiographically occult vascular malformations. Neurosurg Clin N Am. 1999; Jul. 10(3):419–32.10. Saito Y, Kobayashi N. Cerebral venous angiomas: clinical evaluation and possible etiology. Radiology. 1981; Apr. 139(1):87–94.11. Sanmillan JL, Fernández-Coello A, Fernández-Conejero I, Plans G, Gabarrós A. Functional approach using intraoperative brain mapping and neurophysiological monitoring for the surgical treatment of brain metastases in the central region. J Neurosurg. 2017; Mar. 126(3):698–707.12. Sarwar M, McCormick WF. Intracerebral venous angioma. Arch Neurol. 1978; May. 35(5):323–5.13. Walter J, Kuhn SA, Waschke A, Kalff R, Ewald C. Operative treatment of subcortical metastatic tumours in the central region. J Neurooncol. 2011; Jul. 103(3):567–73.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Developmental Venous Anomaly Presenting Intracranial Hemorrhage without Associated Vascular Anomaly
- Repeated Intracerebral Hemorrhage from Developmental Venous Anomaly Alone
- Atypical Developmental Venous Anomaly Associated with Single Arteriovenous Fistula and Intracerebral Hemorrhage: a Case Demonstrated by Superselective Angiography
- Joubert Syndrome Presenting With Normal Pyramidal Decussation: A Case Report
- Cerebellar Dysfunctions Associated with a Developmental Venous Anomaly
