Modified Transosseous Suture Technique for the Quadriceps Avulsion Fracture in Chronic Renal Failure: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Sung-Ae Hospital, Seoul, Korea
- KMID: 2545831
- DOI: http://doi.org/10.5763/kjsm.2023.41.3.163
Abstract
- In patients with chronic renal failure, spontaneous tendon rupture may occur due to degenerative changes in the tendon. Transosseous suture and suture anchor are commonly used for repair of quadriceps tendon rupture. But in chronic renal failure patients, the fixation of the repaired tendon is weak due to degenerative changes in the tendon, and decreased bone mineral density results in a relatively high rerupture rate. In this case, spontaneous quadriceps tendon rupture in a patient who has chronic renal failure with dialysis over 10 years was repaired with a newly designed transosseous suture method in order to increase contact of patella base and to reduce the rate of rerupture. Divide ruptured tendon arbitrarily into four layers using the anatomical structure of quadriceps tendon, then pull them out through the three vertical transosseous tunnels and tied them each. This procedure may be considered as another option in the case with high rerupture risk.
Figure
-
Fig. 1 Preoperative gross clinical photograph that shows swelling of left knee joint without external wound.

Fig. 2 Preoperative lateral plain radiography (A) and computer tomography (B) of the left knee show mild inferior displacement of patella (patella baja Insall-Salvati ratio, 0.71) with avulsion bone fragment (arrows).

Fig. 3 Sagittal view of T2-weighted magnetic resonance imaging shows complete rupture of the quadriceps tendon and massive hemorrhage.
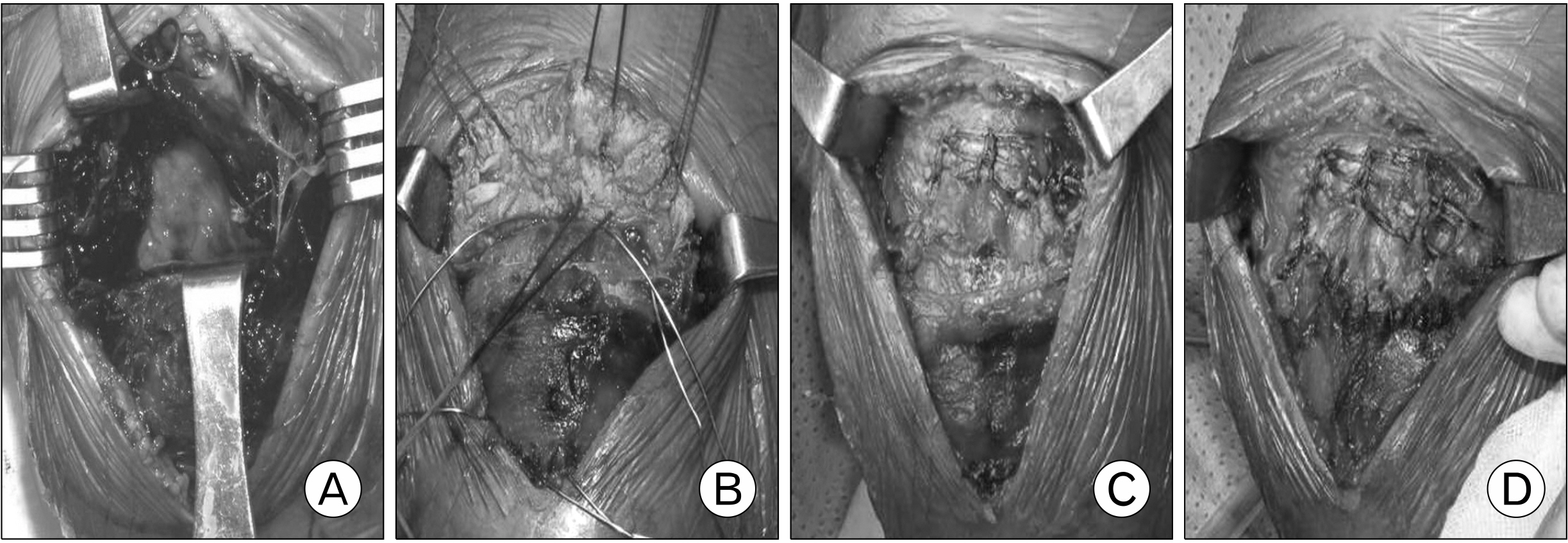
Fig. 4 Intraoperative findings. (A) The quadriceps tendon and extensor retinaculum were ruptured completely, and a massive hematoma was infiltrated. (B) The ruptured quadriceps tendon was divided arbitrarily into four layers. The medial, superior, and lateral portions were sutured using the Krackow technique and the intermediate portion was sutured using the Mason-Allen technique. (C) A transosseous suture was done via three vertical transosseous tunnels. (D) The extensor retinaculum and capsules were sutured.
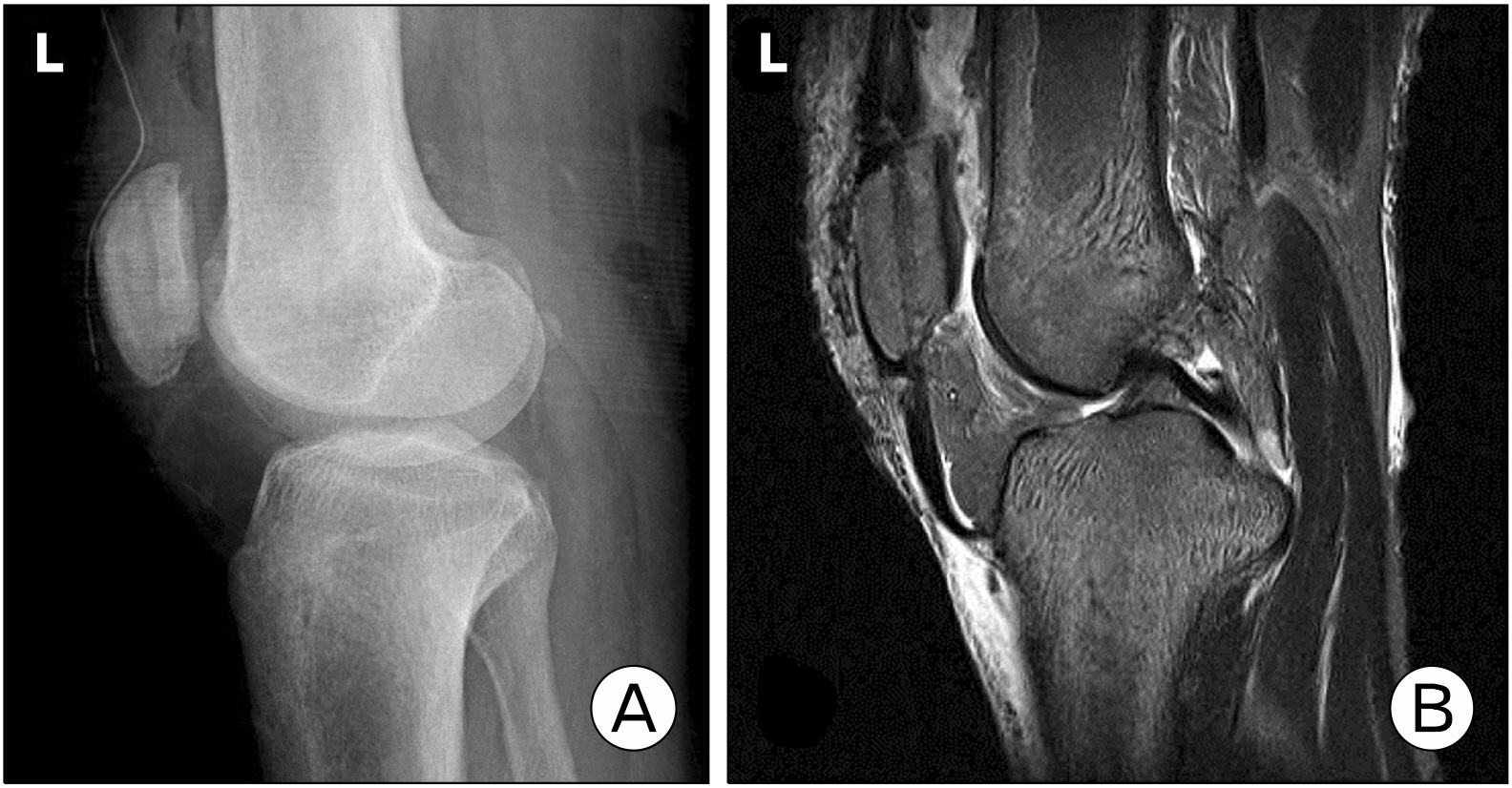
Fig. 5 (A) Inferior displacement of patella was corrected in the postoperative lateral plane. (B) T2-weighted image shows repaired quadriceps tendon and the tendon is attached to the whole surface of patella.
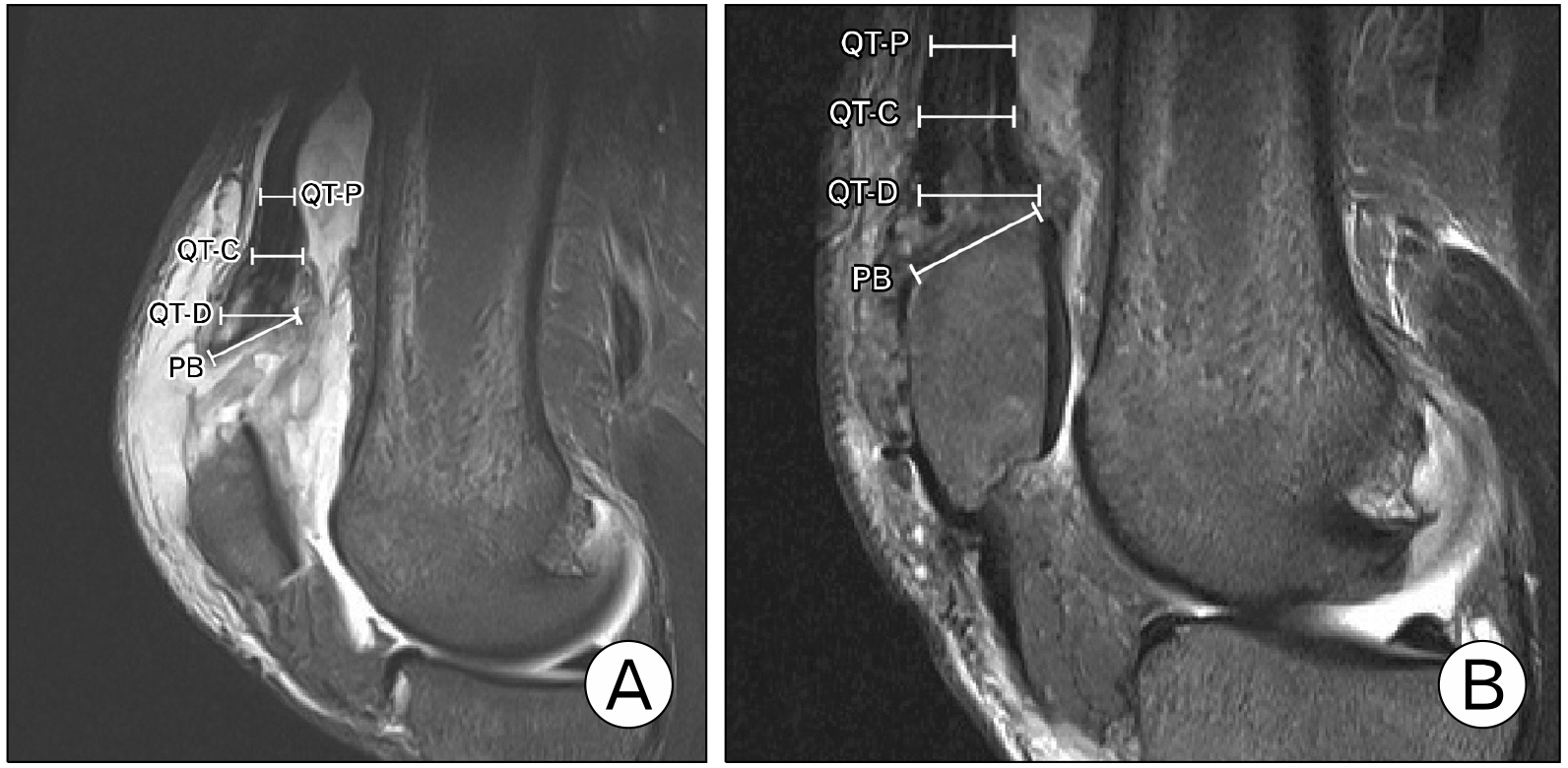
Fig. 6 Quadriceps tendon (QT) measurements from preoperative (A) and postoperative (B) magnetic resonance images. Lines showpredetermined locations for measurements: proximal (QT-P), central (QT-C), distal (QT-D), and patellar base (PB).

Fig. 7 Patient’s postoperative status. The patient regained active extension of the left knee without deficit.
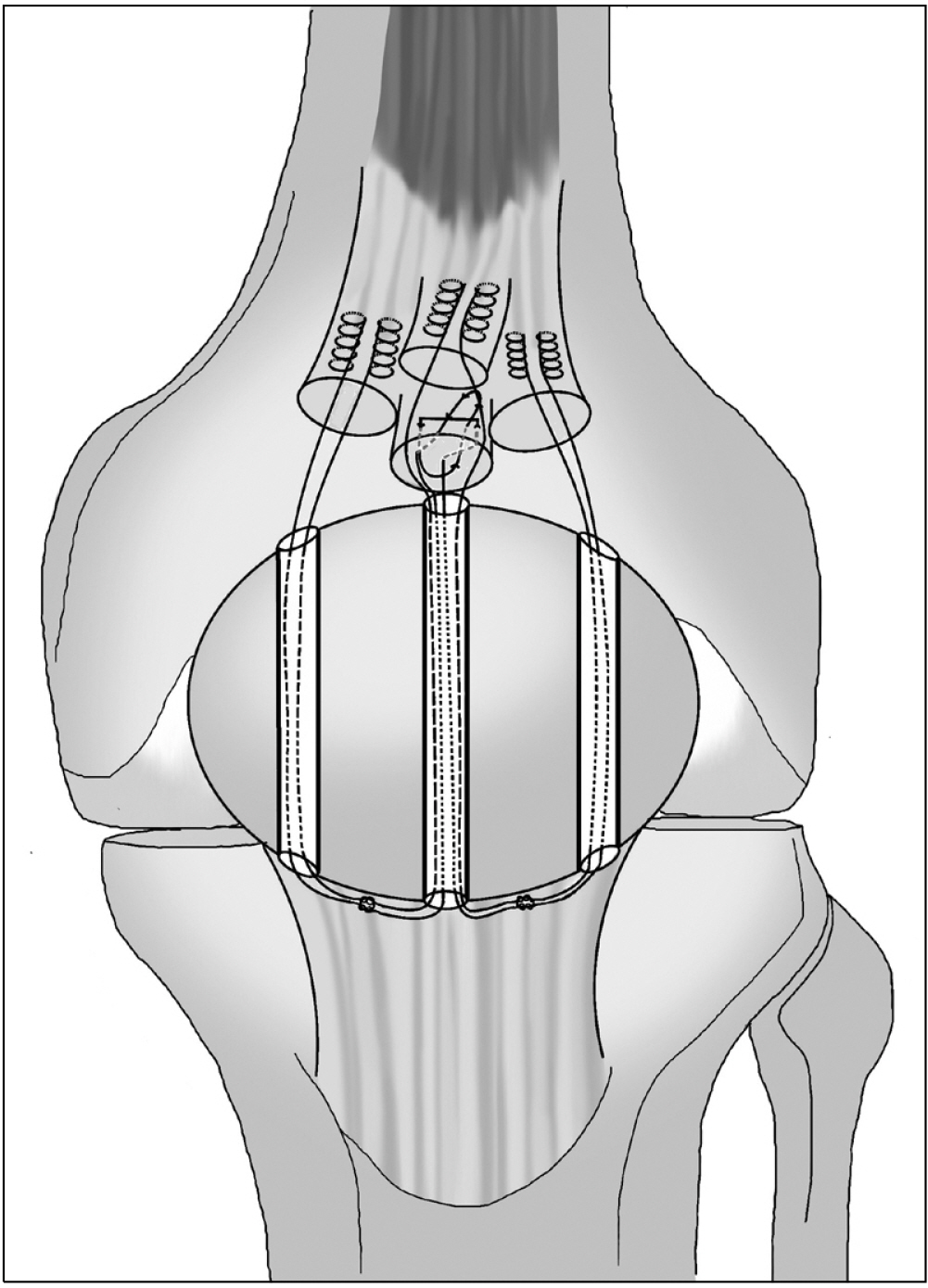
Fig. 8 Illustration of the surgical procedure. The ruptured quadriceps tendon was divided arbitrarily into four layers. The medial, superior, and lateral portions were sutured using the Krackow technique, and the intermediate portion was sutured using the Mason-Allen technique. The sutures were then passed through threevertical parallel tunnels. Fibrowires were tied the knot under the patella.
Reference
-
1. Choi SW, Kim SR, Nam KW, et al. 2010; Spontaneous and simultaneous rupture of bilateral quadriceps tendons in a patient with chronic renal failure. Korean J Sports Med. 28:132–6.2. Kim BS, Kim YW, Song EK, Seon JK, Kang KD, Kim HN. 2012; Simultaneous bilateral quadriceps tendon rupture in a patient with chronic renal failure. Knee Surg Relat Res. 24:56–9. DOI: 10.5792/ksrr.2012.24.1.56. PMID: 22570854. PMCID: PMC3341818.
Article3. Ciriello V, Gudipati S, Tosounidis T, Soucacos PN, Giannoudis PV. 2012; Clinical outcomes after repair of quadriceps tendon rupture: a systematic review. Injury. 43:1931–8. DOI: 10.1016/j.injury.2012.08.044. PMID: 22959496.
Article4. Hochheim MC, Bartels EM, Iversen JV. 2019; Quadriceps tendon rupture. Anchor or transosseous suture? A systematic review. Muscles Ligaments Tendons J. 9:356–62. DOI: 10.32098/mltj.03.2019.09.5. Mehta AV, Wilson C, King TS, Gallo RA. 2021; Outcomes following quadriceps tendon repair using transosseous tunnels versus suture anchors: a systematic review. Injury. 52:339–44. DOI: 10.1016/j.injury.2020.10.020. PMID: 33041016.
Article6. Shah MK. 2002; Simultaneous bilateral quadriceps tendon rupture in renal patients. Clin Nephrol. 58:118–21. DOI: 10.5414/CNP58118. PMID: 12227683.
Article7. Grob K, Manestar M, Filgueira L, Ackland T, Gilbey H, Kuster MS. 2016; New insight in the architecture of the quadriceps tendon. J Exp Orthop. 3:32. DOI: 10.1186/s40634-016-0068-y. PMID: 27813020. PMCID: PMC5095096.8. Flores DV, Mejía Gómez C, Pathria MN. 2018; Layered approach to the anterior knee: normal anatomy and disorders associated with anterior knee pain. Radiographics. 38:2069–101. DOI: 10.1148/rg.2018180048. PMID: 30422763.9. Verdano MA, Zanelli M, Aliani D, Corsini T, Pellegrini A, Ceccarelli F. 2014; Quadriceps tendon tear rupture in healthy patients treated with patellar drilling holes: clinical and ultrasonographic analysis after 36 months of follow-up. Muscles Ligaments Tendons J. 4:194–200. DOI: 10.32098/mltj.02.2014.19. PMID: 25332935. PMCID: PMC4187582.10. Staeubli HU, Bollmann C, Kreutz R, Becker W, Rauschning W. 1999; Quantification of intact quadriceps tendon, quadriceps tendon insertion, and suprapatellar fat pad: MR arthrography, anatomy, and cryosections in the sagittal plane. AJR Am J Roentgenol. 173:691–8. DOI: 10.2214/ajr.173.3.10470905. PMID: 10470905.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mini-Plate and Screw Fixation Technique for Comminuted Flexor Digitorum Profundus Avulsion Fracture
- Isolated Avulsion Fracture of the Lesser Tuberosity of the Humerus: A Case Report
- Simultaneous Bilateral Quadriceps Tendon Rupture in a Patient with Chronic Renal Failure
- Spontaneous Rupture of Quadriceps Tendon: Report of four knees
- Osteochondral Avulsion Fracture in Patella after Treatment of Abscess around Knee: A Case report
