The Effects of Various Maxillary Sinus Antrostomy Techniques on Modifying the Ventilation and Air-Conditioning Characteristics of the Maxillary Sinus: A Numerical Study
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Republic of Korea
- 2Department of Mechanical Engineering, Konkuk University, Seoul, Republic of Korea
- KMID: 2544618
- DOI: http://doi.org/10.18787/jr.2023.00027
Abstract
- Background and Objectives
Endoscopic sinus surgery is commonly performed for maxillary sinus (MS) disease, and the surgical extent of the MS medial wall or ostium varies. We examined the effect of MS surgery on nasal airflow and air-conditioning using computational fluid dynamics in five nasal cavity numerical models.
Methods
Four types of unilateral virtual MS surgery were conducted on the right MS based on computed tomography images of a 49-year-old man with normal anatomy. The five models were as follows: baseline (normal), middle meatal antrostomy (MMA), MMA with inferior meatal antrostomy (MMA+IMA), mega-antrostomy (MEGA), and endoscopic medial maxillectomy (EMM). Virtual simulator software and a stereoscopic display with haptic device were used for virtual surgery. Meshing software and computer fluid dynamics software were used to generate meshes and analyze airflow.
Results
The MMA and MMA+IMA results were similar to the baseline model. However, EMM and MEGA exhibited some physiological changes. The amount of airflow moving into the MS was largest in the EMM model, followed by the MEGA model. The distributions of wall shear stress and surface water-vapor increased near the enlarged MS ostium in EMM and MEGA. Skewed airflow partition and different airflow rates between the operated and unoperated sites of the nose also changed the air-conditioning characteristics. EMM substantially reduced the relative humidity in the nasopharynx, and MEGA showed a smaller reduction.
Conclusion
Among four surgery techniques, EMM produced the largest increase in wall shear stress and surface water vapor flux on the posterior surface of the MS and the greatest deterioration in the nasal cavity’s air-conditioning capacity. MEGA reduced the local airflow disturbance inside the MS and prevented excessive degeneration of the cavity’s overall air-conditioning capacity. In conclusion, MEGA and modified EMM approaches have physiological advantages over EMM, while securing a sufficient spatial extent of resection for surgery.
Keyword
Figure
-
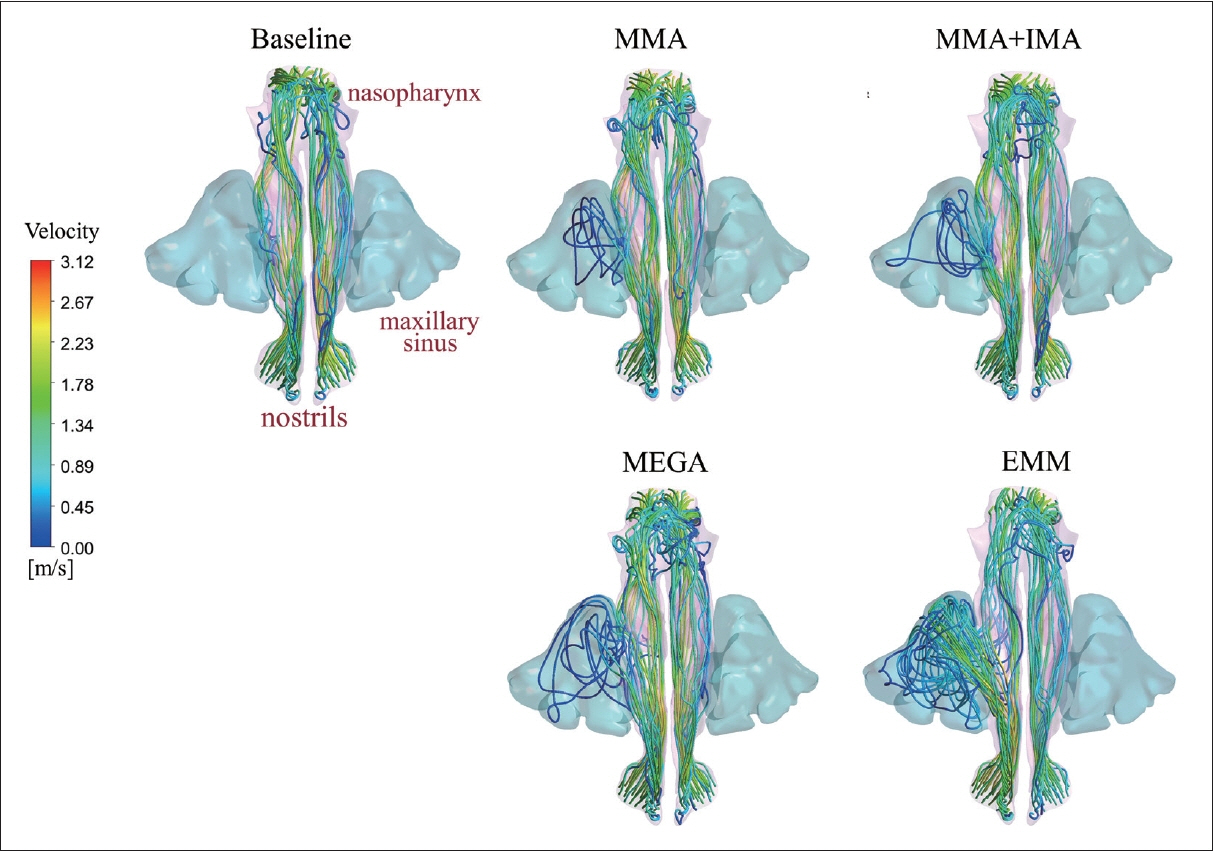
Fig. 1. Comparison of streamline patterns between five models. For visual convenience, the face was removed. Streamline patterns of airflow illustrate that the degree of ventilation of MS was different according to the operation technique. The infiltration of the airflow into the right MS was negligibly small in the baseline model. Weak permeation was observed in the MMA model, but limited to the region near the enlarged ostium. The degree of penetration of the airflow became even larger in the MMA+IMA and MEGA models. Complete penetration in the right MS was noted in the EMM model. MMA, middle meatal antrostomy; IMA, inferior meatal antrostomy; MEGA, megaantrostomy; MS, maxillary sinus; EMM, endoscopic medial maxillectomy.

Fig. 2. Comparison of velocity distributions along the nasal airway in five representative coronal planes. The bilateral airflow velocity magnitude is shown by five representative planes from the anterior part to the posterior part. In the baseline model, the velocity inside the MS was very low, with a maximum velocity less than 0.01 m/s. However, disturbed velocity regions were found near the enlarged ostium or medial wall of the right MS in the MMA, MMA+IMA, and MEGA models, and the maximum velocity near these regions was approximately 0.91, 1.42, and 0.82 m/s in the MMA, MMA+IMA, and MEGA models, respectively. In the EMM model, a drastically increased level of disturbance inside the right MS was found, with a maximum velocity of 2.03 m/s near the extended ostium connected to the middle meatus. MS, maxillary sinus; MMA, middle meatal antrostomy; IMA, inferior meatal antrostomy; MEGA, mega-antrostomy; EMM, endoscopic medial maxillectomy.
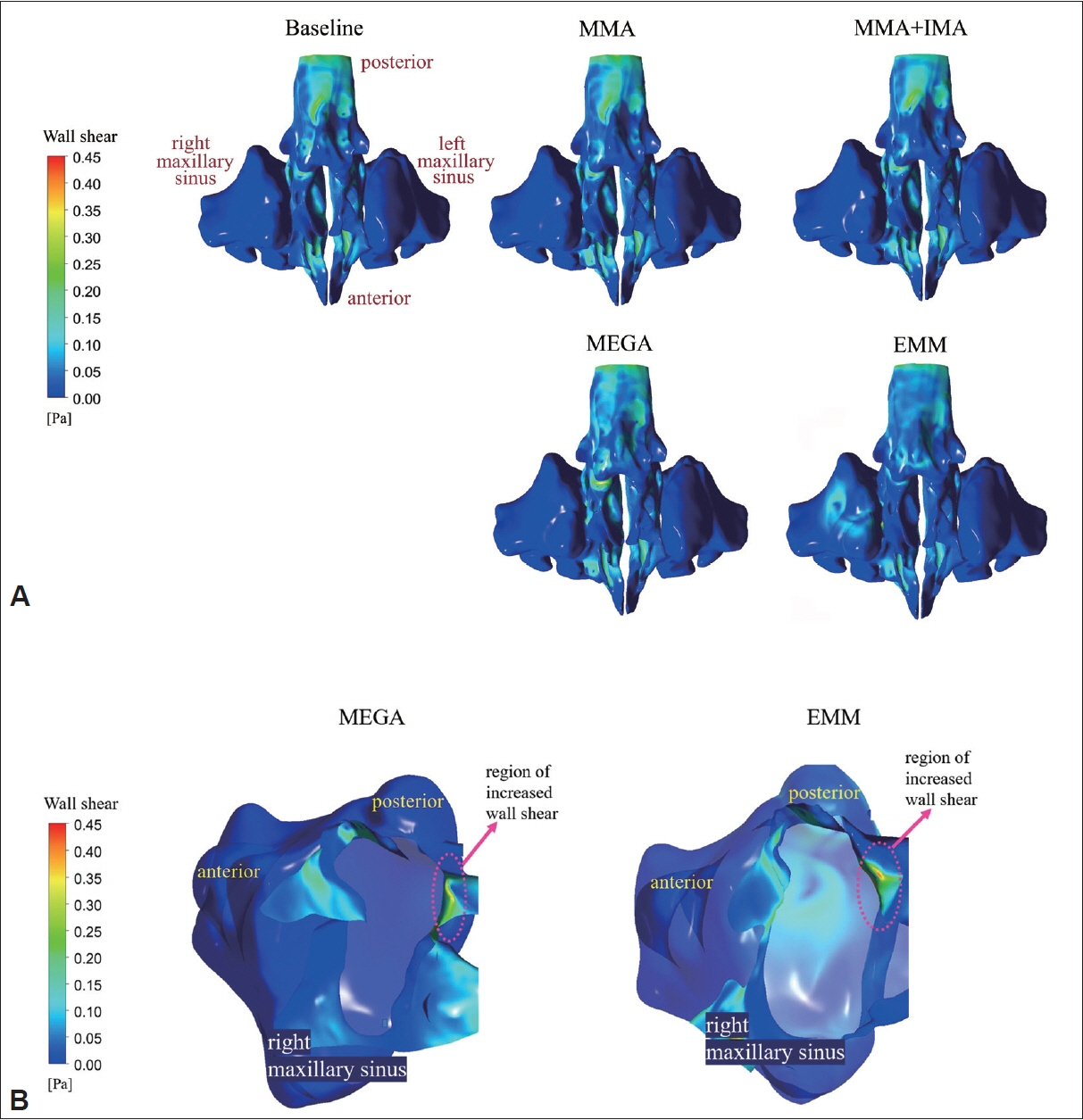
Fig. 3. Comparison of wall shear stress distributions between five models. A: Overall distribution of wall shear stress in five models. In the baseline model, the nasal valve area was subject to high wall shear stress, and a maximum wall shear stress of 0.494 Pa was observed. From the epithelial surface of the MS in the baseline model, vanishingly small wall shear stress was measured. In the MMA, MMA+IMA, and MEGA models, the wall shear stress at the surface of the right MS remained small. However, in the EMM model, a region exposed to elevated wall shear stress appeared at the posterior surface of the right MS. B: The distribution of wall shear stress near the extended ostium in the MEGA and EMM models. For visual purposes, the cavity connected to the right MS was artificially removed. In the MEGA model, the wall shear stress at the posterior surface of the enlarged ostium increased to approximately 0.364 Pa. In the EMM model, a higher value of wall shear stress (approximately 0.412 Pa) was noted in the posterior surface of the enlarged ostium. In addition, the EMM model showed increased wall shear stress (approximately 0.155 Pa) at the posterior surface of the right MS. MS, maxillary sinus; MMA, middle meatal antrostomy; IMA, inferior meatal antrostomy; MEGA, mega-antrostomy; EMM, endoscopic medial maxillectomy.
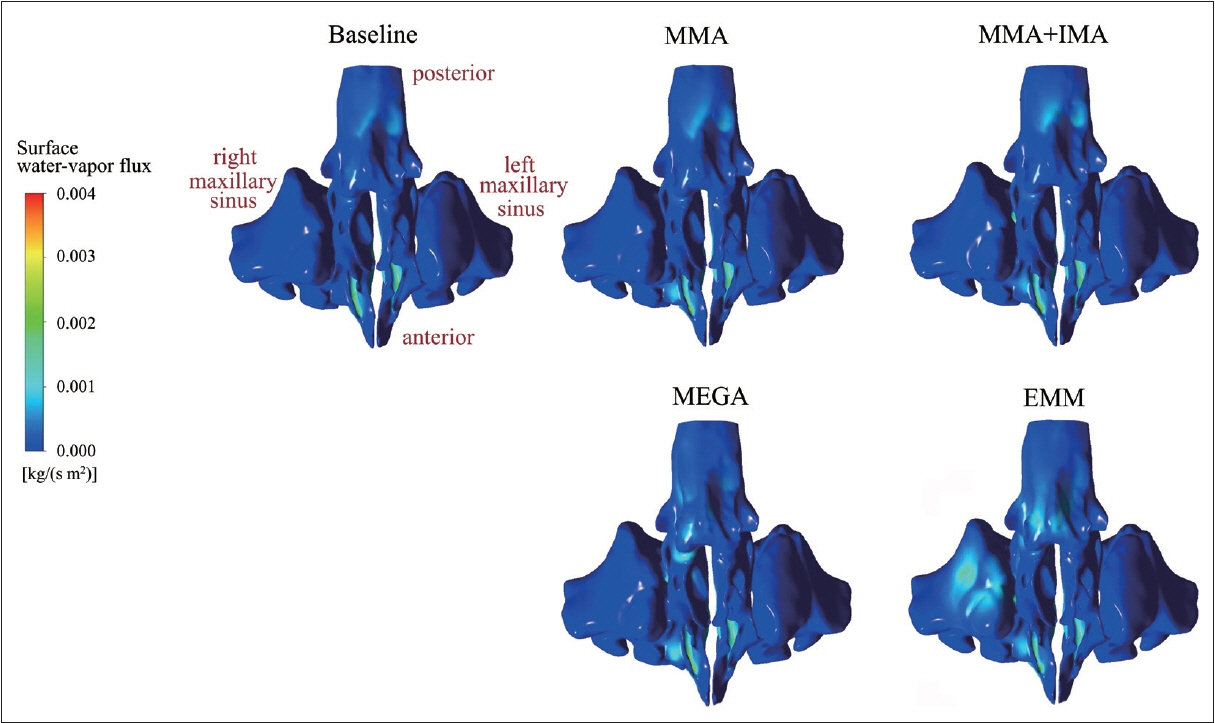
Fig. 4. Comparison of epithelial surface water-vapor flux distributions between five models. In the MMA, MMA+IMA, and MEGA models, there were no noticeable changes in water-vapor flux along the surface of the right MS. In the EMM model, however, the water-vapor flux on the posterior surface of the right MS increased to approximately 1.60×10-3 kg/(s·m2). MMA, middle meatal antrostomy; IMA, inferior meatal antrostomy; MEGA, mega-antrostomy; MS, maxillary sinus; EMM, endoscopic medial maxillectomy.
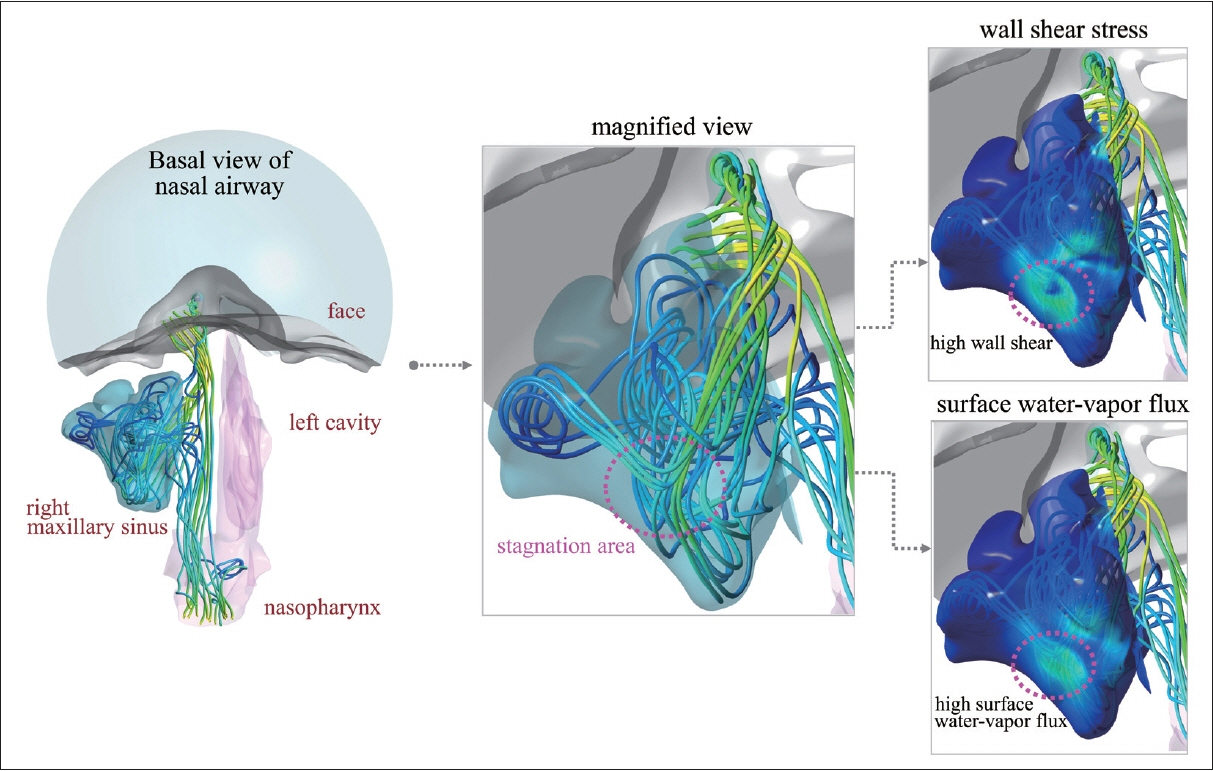
Fig. 5. Stagnation in the posterior surface of the maxillary sinus of the EMM model. A large portion of the airflow from the right nostril entered the right maxillary sinus. A bulk of penetrating airflow proceeded before colliding with the posterior surface of the right maxillary sinus. Therefore, a stagnation area was formed on the posterior surface of the maxillary sinus where the wall shear stress and surface water- vapor flux increased. For visual convenience, only the airflow through the right nasal cavity was considered and the surface of the right maxillary sinus was made semi-transparent. EMM, endoscopic medial maxillectomy.
Reference
-
References
1. Osguthorpe JD, Weisman RA. ‘Medial maxillectomy’ for lateral nasal wall neoplasms. Arch Otolaryngol Head Neck Surg. 1991; 117(7):751–6.2. Kennedy DW, Adappa ND. Endoscopic maxillary antrostomy: not just a simple procedure. Laryngoscope. 2011; 121(10):2142–5.3. Tan J, Han D, Wang J, Liu T, Wang T, Zang H, et al. Numerical simulation of normal nasal cavity airflow in Chinese adult: a computational flow dynamics model. Eur Arch Otorhinolaryngol. 2012; 269(3):881–9.4. Weber RK, Werner JA, Hildenbrand T. Endonasal endoscopic medial maxillectomy with preservation of the inferior turbinate. Am J Rhinol Allergy. 2010; 24(6):132–5.5. Lindemann J, Keck T, Wiesmiller K, Sander B, Brambs HJ, Rettinger G, et al. Nasal air temperature and airflow during respiration in numerical simulation based on multislice computed tomography scan. Am J Rhinol. 2006; 20(2):219–23.6. Garcia GJ, Bailie N, Martins DA, Kimbell JS. Atrophic rhinitis: a CFD study of air conditioning in the nasal cavity. J Appl Physiol (1985). 2007; 103(3):1082–92.7. Kim DW, Chung SK, Na Y. Numerical study on the air conditioning characteristics of the human nasal cavity. Comput Biol Med. 2017; 86:18–30.8. Ashman A, Psaltis AJ, Wormald PJ, Tan NC. Extended endoscopic approaches to the maxillary sinus. J Laryngol Otol. 2020; 134(6):473–80.9. Doorly DJ, Taylor DJ, Schroter RC. Mechanics of airflow in the human nasal airways. Respir Physiol Neurobiol. 2008; 163(1-3):100–10.10. Chung SK, Jo G, Kim SK, Na Y. The effect of a middle meatal antrostomy on nitric oxide ventilation in the maxillary sinus. Respir Physiol Neurobiol. 2014; 192:7–16.11. Burgos MA, Sanmiguel-Rojas E, Martín-Alcántara A, Hidalgo-Martínez M. Effects of the ambient temperature on the airflow across a Caucasian nasal cavity. Int J Numer Method Biomed Eng. 2014; 30(3):430–45.12. Inthavong K, Ma J, Shang Y, Dong J, Chetty ASR, Tu J, et al. Geometry and airflow dynamics analysis in the nasal cavity during inhalation. Clin Biomech (Bristol, Avon). 2019; 66:97–106.13. Chung SK, Na Y. Dynamic characteristics of heat capacity of the human nasal cavity during a respiratory cycle. Respir Physiol Neurobiol. 2021; 290:103674.14. Xiong GX, Zhan JM, Zuo KJ, Rong LW, Li JF, Xu G. Use of computational fluid dynamics to study the influence of the uncinate process on nasal airflow. J Laryngol Otol. 2011; 125(1):30–7.15. Leong SC, Chen XB, Lee HP, Wang DY. A review of the implications of computational fluid dynamic studies on nasal airflow and physiology. Rhinology. 2010; 48(2):139–45.16. Won TB, Cho SW, Sung MW, Paek SH, Chan S, Salisbury K, et al. Validation of a rhinologic virtual surgical simulator for performing a Draf 3 endoscopic frontal sinusotomy. Int Forum Allergy Rhinol. 2019; 9(8):910–7.17. Abouali O, Keshavarzian E, Farhadi Ghalati P, Faramarzi A, Ahmadi G, Bagheri MH. Micro and nanoparticle deposition in human nasal passage pre and post virtual maxillary sinus endoscopic surgery. Respir Physiol Neurobiol. 2012; 181(3):335–45.18. Lindemann J, Keck T, Wiesmiller K, Sander B, Brambs HJ, Rettinger G, et al. A numerical simulation of intranasal air temperature during inspiration. Laryngoscope. 2004; 114(6):1037–41.19. International Commission on Radiological Protection. Human respiratory tract model for radiological protection. Ann ICRP. 1994; 24(1-3):1–482.20. Costa ML, Psaltis AJ, Nayak JV, Hwang PH. Long-term outcomes of endoscopic maxillary mega-antrostomy for refractory chronic maxillary sinusitis. Int Forum Allergy Rhinol. 2015; 5(1):60–5.21. Cho DY, Hwang PH. Results of endoscopic maxillary mega-antrostomy in recalcitrant maxillary sinusitis. Am J Rhinol. 2008; 22(6):658–62.22. Kennedy DW, Shaalan H. Reevaluation of maxillary sinus surgery: experimental study in rabbits. Ann Otol Rhinol Laryngol. 1989; 98(11):901–6.23. Suzuki M, Nakamura Y, Yokota M, Ozaki S, Murakami S. Modified transnasal endoscopic medial maxillectomy through prelacrimal duct approach. Laryngoscope. 2017; 127(10):2205–9.24. Lundberg JO. Nitric oxide and the paranasal sinuses. Anat Rec (Hoboken). 2008; 291(11):1479–84.25. Zhang J, Sun Y, Liu M, Sun C, Tian L. Predictive and diagnostic value of fractional exhaled nitric oxide in patients with chronic rhinosinusitis. Med Sci Monit. 2019; 25:150–6.26. Kirihene RK, Rees G, Wormald PJ. The influence of the size of the maxillary sinus ostium on the nasal and sinus nitric oxide levels. Am J Rhinol. 2002; 16(5):261–4.27. Saibene AM, Felisati G, Pipolo C, Bulfamante AM, Quadrio M, Covello V. Partial preservation of the inferior turbinate in endoscopic medial maxillectomy: a computational fluid dynamics study. Am J Rhinol Allergy. 2020; 34(3):409–16.28. Eccles R, Jones AS. The effect of menthol on nasal resistance to air flow. J Laryngol Otol. 1983; 97(8):705–9.29. Jones AS, Crosher R, Wight RG, Lancer JM, Beckingham E. The effect of local anaesthesia of the nasal vestibule on nasal sensation of airflow and nasal resistance. Clin Otolaryngol Allied Sci. 1987; 12(6):461–4.30. Malik J, Spector BM, Wu Z, Markley J, Zhao S, Otto BA, et al. Evidence of nasal cooling and sensory impairments driving patient symptoms with septal deviation. Laryngoscope. 2022; 132(3):509–17.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Characteristics According to the Radiological Classifications of Maxillary Sinus Fungus Ball
- Long-Term Outcomes of Transnasal Endoscopic Marsupialization through Middle, Inferior Meatal Antrostomy or Extended Middle Meatal Antrostomy in Maxillary Sinus Mucoceles
- Sinusitis Managment Associated with Maxillary Sinus Augmentation: Case Report
- Bilateral Pneumosinus Dilatans of the Maxillary Sinuses with Facial Pain
- Anthropometric Characteristics of the Maxillary Sinus in Korean
