Ann Surg Treat Res.
2023 Jul;105(1):57-62. 10.4174/astr.2023.105.1.57.
Redo pull-through for postoperative complications following pull-through in Hirschsprung disease: a single center experience
- Affiliations
-
- 1Department of Surgery, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea
- 2Division of Pediatric Surgery, Asan Medical Center Children’s Hospital, Department of Surgery, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2544613
- DOI: http://doi.org/10.4174/astr.2023.105.1.57
Abstract
- Purpose
Although surgical management of Hirschsprung disease (HD) is effective in most patients, some patients experience long-term postoperative complications, and require redo pull-through (PT). The present study evaluated clinical outcomes of redo PT in HD patients at a single center.
Methods
Patients with HD who underwent redo PT procedures between 2003 and 2019 were retrospectively reviewed.
Results
Thirteen patients were included. Five (38.5%) had undergone initial PT surgery at our center and 8 (61.5%) at other centers. Redo PT procedures were transanal endorectal PT in 12 patients (92.3%) and the posterior sagittal approach in 1 patient (7.7%). Indications for redo PT included pathologic misdiagnosis in 8 patients (61.5%); stricture in 2 (15.4%); and rectal stenosis, obstructing Duhamel pouch and remnant septum in 1 each (7.7%). At a median follow-up of 68 months (range, 3–227 months) after redo PT, 8 patients (61.5%) had normal bowel function, 2 (15.4%) had incontinence, and 1 (7.7%) had constipation.
Conclusion
Redo PT procedures could be an effective approach for improving obstructive symptoms in HD patients with anatomic or pathologic reasons following primary PT. Careful selection of patients and discreet indications for redo PT are crucial.
Figure
-

Fig. 1 Contrast enema of a patient who had a Duhamel procedure. The enlarged Duhamel pouch was causing obstructive symptoms.
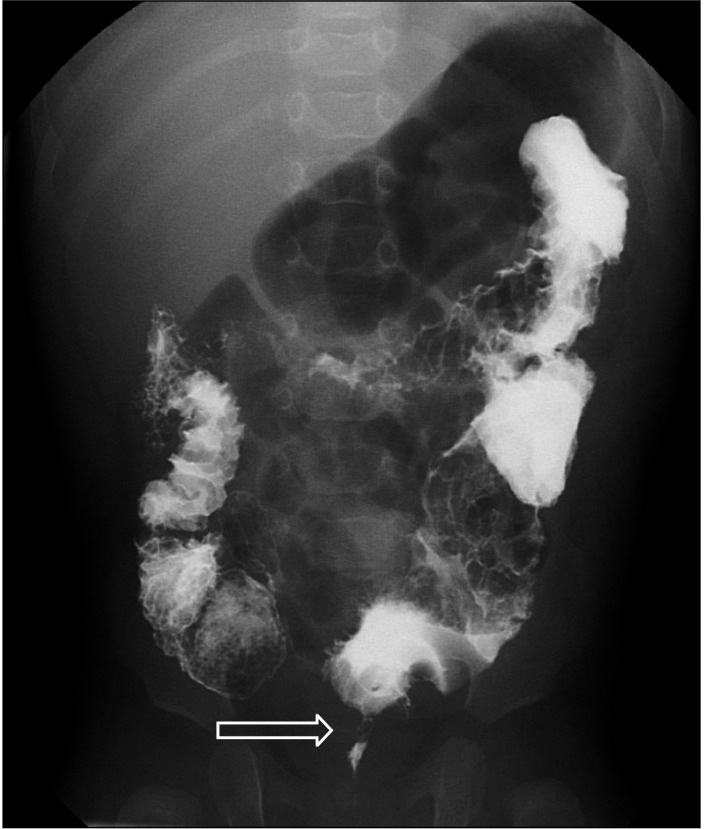
Fig. 2 Contrast enema of a patient with retained aganglionosis after transanal endorectal pull-through. The arrow shows the transition zone.
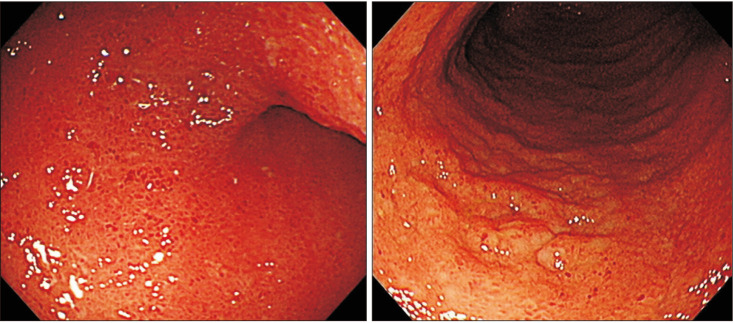
Fig. 3 Endoscopic findings of a patient with total colonic aganglionosis after redo pull-through showing hyperemic mucosa with aphthous ulcers. Endoscopic biopsy reported chronic active ileitis with dense lymphoplasmacytic infiltration in lamina propria and cryptitis.
Reference
-
1. Swenson O, Bill AH Jr. Resection of rectum and rectosigmoid with preservation of the sphincter for benign spastic lesions producing megacolon; an experimental study. Surgery. 1948; 24:212–220. PMID: 18872852.2. Peña A, Elicevik M, Levitt MA. Reoperations in Hirschsprung disease. J Pediatr Surg. 2007; 42:1008–1014. PMID: 17560211.3. Levitt MA, Dickie B, Peña A. Evaluation and treatment of the patient with Hirschsprung disease who is not doing well after a pull-through procedure. Semin Pediatr Surg. 2010; 19:146–153. PMID: 20307851.4. Ahmad H, Yacob D, Halleran DR, Gasior AC, Lorenzo CD, Wood RJ, et al. Evaluation and treatment of the post pull-through Hirschsprung patient who is not doing well; update for 2022. Semin Pediatr Surg. 2022; 31:151164. PMID: 35690463.5. Ralls MW, Coran AG, Teitelbaum DH. Redo pullthrough for Hirschsprung disease. Pediatr Surg Int. 2017; 33:455–460. PMID: 28040830.6. De la Torre-Mondragón L, Ortega-Salgado JA. Transanal endorectal pull-through for Hirschsprung’s disease. J Pediatr Surg. 1998; 33:1283–1286. PMID: 9722005.7. Ralls MW, Coran AG, Teitelbaum DH. Reoperative surgery for Hirschsprung disease. Semin Pediatr Surg. 2012; 21:354–363. PMID: 22985841.8. Lawal TA, Chatoorgoon K, Collins MH, Coe A, Peña A, Levitt MA. Redo pull-through in Hirschsprung’s [corrected] disease for obstructive symptoms due to residual aganglionosis and transition zone bowel. J Pediatr Surg. 2011; 46:342–347. PMID: 21292085.9. Ralls MW, Freeman JJ, Rabah R, Coran AG, Ehrlich PF, Hirschl RB, et al. Redo pullthrough for Hirschsprung disease: a single surgical group’s experience. J Pediatr Surg. 2014; 49:1394–1399. PMID: 25148745.10. Dingemans A, van der Steeg H, Rassouli-Kirchmeier R, Linssen MW, van Rooij I, de Blaauw I. Redo pull-through surgery in Hirschsprung disease: short-term clinical outcome. J Pediatr Surg. 2017; 52:1446–1450. PMID: 27765267.11. Li Q, Zhang Z, Xiao P, Ma Y, Yan Y, Jiang Q, et al. Surgical approach and functional outcome of redo pull-through for postoperative complications in Hirschsprung’s disease. Pediatr Surg Int. 2021; 37:1401–1407. PMID: 34417631.12. Nour S, Beck J, Stringer MD. Colostomy complications in infants and children. Ann R Coll Surg Engl. 1996; 78:526–530. PMID: 8943638.13. Bischoff A, Frischer J, Knod JL, Dickie B, Levitt MA, Holder M, et al. Damaged anal canal as a cause of fecal incontinence after surgical repair for Hirschsprung disease: a preventable and under-reported complication. J Pediatr Surg. 2017; 52:549–553. PMID: 27624566.14. Nakamura H, Lim T, Puri P. Inflammatory bowel disease in patients with Hirschsprung’s disease: a systematic review and meta-analysis. Pediatr Surg Int. 2018; 34:149–154. PMID: 28983688.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Hirschsprung's Disease: Including reoperation and total colonic aganglionosis
- Laparoscopic Primary Endorectal Pull-through Procedure (Boley's) for Hirschsprung's Disease
- Definitive Operation Using Two GIA Autosutures for Hirschsprung's Disease
- Short-Term Outcomes of Transanal One-Stage Pull-Through for Hirschsprung's Disease
- Re-pull-through Operation in Hirschsprung's Disease
