Ann Rehabil Med.
2023 Jun;47(3):205-213. 10.5535/arm.22147.
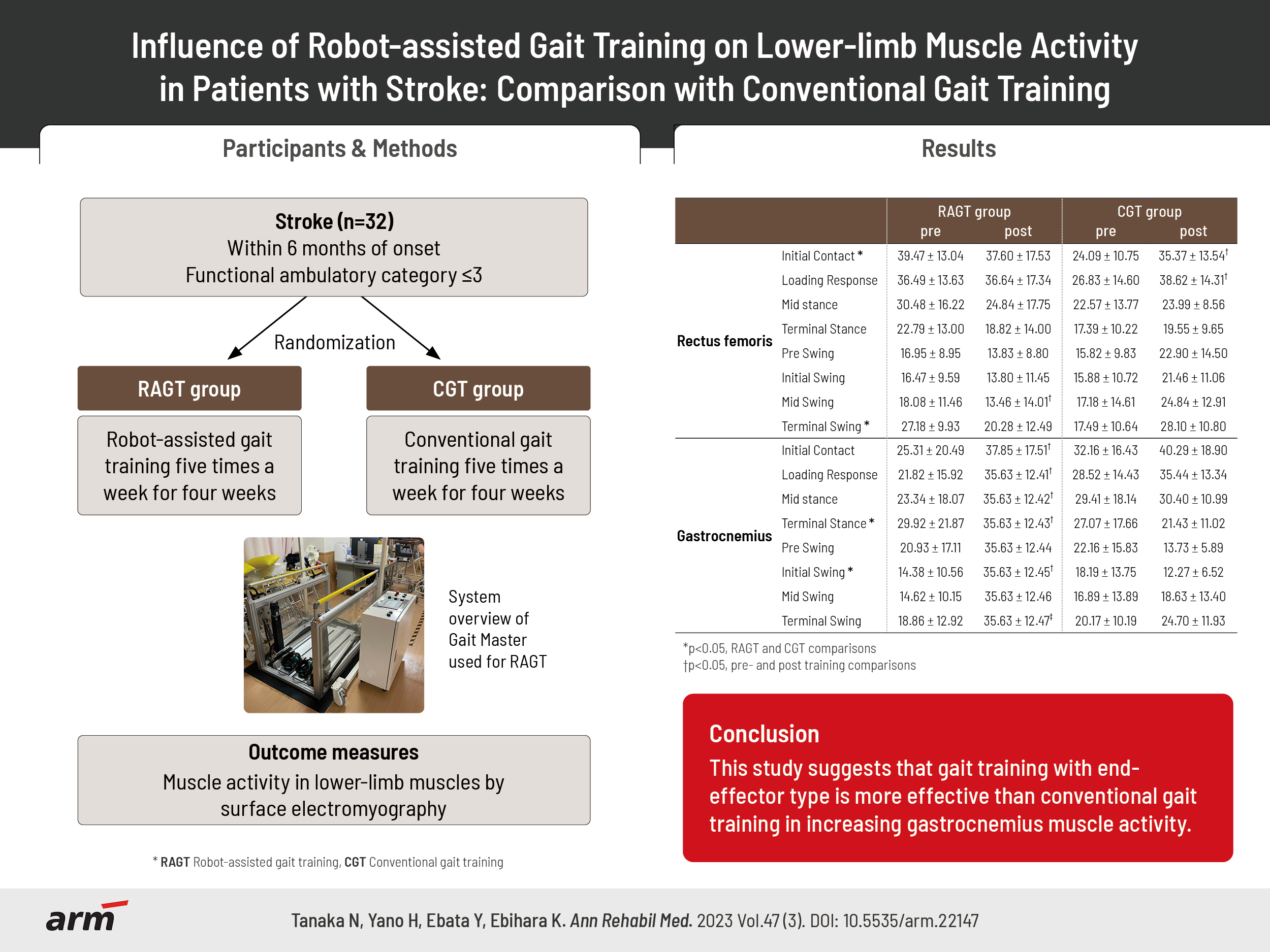
Influence of Robot-Assisted Gait Training on Lower-Limb Muscle Activity in Patients With Stroke: Comparison With Conventional Gait Training
- Affiliations
-
- 1Department of Physical Therapy, School of Rehabilitation, Tokyo Professional University of Health Sciences, Tokyo, Japan
- 2Division of Intelligent Interaction Technologies, Faculty of Engineering, Information and Systems, University of Tsukuba, Tsukuba, Japan
- 3Department of Rehabilitation Medicine, Hitachi, Ltd., Hitachinaka General Hospital, Hitachinaka, Japan
- KMID: 2543417
- DOI: http://doi.org/10.5535/arm.22147
Abstract
Objective
To measure muscle activity before and after robot-assisted gait training (RAGT) in patients with stroke and examine the differences in muscle activity changes compared with conventional gait training (CGT).
Methods
Thirty patients with stroke (RAGT group, n=17; CGT group, n=13) participated in the study. All patients underwent RAGT using a footpad locomotion interface or CGT for 20 minutes for a total of 20 sessions. Outcome measures were lower-limb muscle activity and gait speed. Measurements were performed before the start of the intervention and after the end of the 4-week intervention.
Results
The RAGT group showed increased muscle activity in the gastrocnemius, whereas the CGT group showed high muscle activity in the rectus femoris. In the terminal stance of the gait cycle, the gastrocnemius, the increase in muscle activity was significantly higher in the RAGT group than in the CGT group.
Conclusion
The results suggest that RAGT with end-effector type is more effective than CGT to increase the gastrocnemius muscle activity.
Keyword
Figure
-

Fig. 1. Consort flow chart. FAC, functional ambulation category.
Reference
-
1. Friedman PJ. Gait recovery after hemiplegic stroke. Int Disabil Stud. 1990; 12:119–22.
Article2. Dobkin BH. Clinical practice. Rehabilitation after stroke. N Engl J Med. 2005; 352:1677–84.3. Hesse S, Uhlenbrock D. A mechanized gait trainer for restoration of gait. J Rehabil Res Dev. 2000; 37:701–8.4. Cumming TB, Thrift AG, Collier JM, Churilov L, Dewey HM, Donnan GA, et al. Very early mobilization after stroke fast-tracks return to walking: further results from the phase II AVERT randomized controlled trial. Stroke. 2011; 42:153–8.
Article5. Buesing C, Fisch G, O'Donnell M, Shahidi I, Thomas L, Mummidisetty CK, et al. Effects of a wearable exoskeleton stride management assist system (SMA®) on spatiotemporal gait characteristics in individuals after stroke: a randomized controlled trial. J Neuroeng Rehabil. 2015; 12:69.
Article6. Colombo G, Wirz M, Dietz V. Driven gait orthosis for improvement of locomotor training in paraplegic patients. Spinal Cord. 2001; 39:252–5.
Article7. Jezernik S, Colombo G, Keller T, Frueh H, Morari M. Robotic orthosis lokomat: a rehabilitation and research tool. Neuromodulation. 2003; 6:108–15.
Article8. Husemann B, Müller F, Krewer C, Heller S, Koenig E. Effects of locomotion training with assistance of a robot-driven gait orthosis in hemiparetic patients after stroke: a randomized controlled pilot study. Stroke. 2007; 38:349–54.
Article9. Mayr A, Kofler M, Quirbach E, Matzak H, Fröhlich K, Saltuari L. Prospective, blinded, randomized crossover study of gait rehabilitation in stroke patients using the Lokomat gait orthosis. Neurorehabil Neural Repair. 2007; 21:307–14.
Article10. van Nunen MP, Gerrits KH, Konijnenbelt M, Janssen TW, de Haan A. Recovery of walking ability using a robotic device in subacute stroke patients: a randomized controlled study. Disabil Rehabil Assist Technol. 2015; 10:141–8.
Article11. Yano H, Kasai K, Saitou H, Iwata H. Development of a gait rehabilitation system using a locomotion interface. J Visual Comput Animat. 2003; 14:243–52.
Article12. Yano H, Tamefusa S, Tanaka N, Saito H, Iwata H. Interactive gait rehabilitation system with a locomotion interface for training patients to climb stairs. Presence. 2012; 21:16–30.
Article13. Tanaka N, Saitou H, Takao T, Iizuka N, Okuno J, Yano H, et al. Effects of gait rehabilitation with a footpad-type locomotion interface in patients with chronic post-stroke hemiparesis: a pilot study. Clin Rehabil. 2012; 26:686–95.
Article14. Yano H, Tanaka N, Kamibayashi K, Saitou H, Iwata H. Development of a portable gait rehabilitation system for home-visit rehabilitation. ScientificWorldJournal. 2015; 2015:849831.
Article15. Schwartz I, Sajin A, Fisher I, Neeb M, Shochina M, Katz-Leurer M, et al. The effectiveness of locomotor therapy using robotic-assisted gait training in subacute stroke patients: a randomized controlled trial. PM R. 2009; 1:516–23.
Article16. Tanaka N, Ebihara K, Ebata Y, Yano H. Effect of gait rehabilitation with a footpad-type locomotion interface on gait ability in subacute stroke patients. NeuroRehabilitation. 2022; 50:401–7.
Article17. Molteni F, Gasperini G, Cannaviello G, Guanziroli E. Exoskeleton and end-effector robots for upper and lower limbs rehabilitation: narrative review. PM R. 2018; 10(9 Suppl 2):S174–88.
Article18. Goffredo M, Iacovelli C, Russo E, Pournajaf S, Di Blasi C, Galafate D, et al. Stroke gait rehabilitation: a comparison of end-effector, overground exoskeleton, and conventional gait training. Appl Sci. 2019; 9:2627.
Article19. Lee HJ, Lee SH, Seo K, Lee M, Chang WH, Choi BO, et al. Training for walking efficiency with a wearable hip-assist robot in patients with stroke: a pilot randomized controlled trial. Stroke. 2019; 50:3545–52.
Article20. Mehrholz J, Thomas S, Werner C, Kugler J, Pohl M, Elsner B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev. 2017; 5:CD006185.21. Hidler J, Nichols D, Pelliccio M, Brady K, Campbell DD, Kahn JH, et al. Multicenter randomized clinical trial evaluating the effectiveness of the Lokomat in subacute stroke. Neurorehabil Neural Repair. 2009; 23:5–13.22. Hornby TG, Campbell DD, Kahn JH, Demott T, Moore JL, Roth HR. Enhanced gait-related improvements after therapist- versus robotic-assisted locomotor training in subjects with chronic stroke: a randomized controlled study. Stroke. 2008; 39:1786–92. Erratum in: Stroke 2008;39:e143.23. Mayr A, Quirbach E, Picelli A, Kofler M, Smania N, Saltuari L. Early robot-assisted gait retraining in non-ambulatory patients with stroke: a single blind randomized controlled trial. Eur J Phys Rehabil Med. 2018; 54:819–26.24. Federici S, Meloni F, Bracalenti M, De Filippis ML. The effectiveness of powered, active lower limb exoskeletons in neurorehabilitation: a systematic review. NeuroRehabilitation. 2015; 37:321–40.25. Hidler JM, Wall AE. Alterations in muscle activation patterns during robotic-assisted walking. Clin Biomech (Bristol, Avon). 2005; 20:184–93.26. Coenen P, van Werven G, van Nunen MP, Van Dieën JH, Gerrits KH, Janssen TW. Robot-assisted walking vs overground walking in stroke patients: an evaluation of muscle activity. J Rehabil Med. 2012; 44:331–7.
Article27. Holden MK, Gill KM, Magliozzi MR, Nathan J, Piehl-Baker L. Clinical gait assessment in the neurologically impaired. Reliability and meaningfulness. Phys Ther. 1984; 64:35–40.28. Chacko KA. AHA Medical/Scientific Statement: 1994 revisions to classification of functional capacity and objective assessment of patients with diseases of the heart. Circulation. 1995; 92:2003–5.29. Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975; 12:189–98.30. Iwata H, Yano H, Nakaizumi F. Gait Master: a versatile locomotion interface for uneven virtual terrain. Paper presented at: IEEE Virtual Reality 2001; 2001 Mar 13-17; Yokohama, Japan.31. Yano H, Tamefusa S, Tanaka N, Saitou H, Iwata H. Gait rehabilitation for stair climbing with a locomotion interface. Paper presented at: 2009 IEEE International Conference on Rehabilitation Robotics; 2009 Jun 23-26; Kyoto, Japan.32. Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol. 2000; 10:361–74.
Article33. Perry J, Burnfield J. Gait analysis: normal and pathological function. 2nd ed. West Deptford: Slack Incorporated;2010. p. 4–16.34. Prosser LA, Stanley CJ, Norman TL, Park HS, Damiano DL. Comparison of elliptical training, stationary cycling, treadmill walking and overground walking. Electromyographic patterns. Gait Posture. 2011; 33:244–50.
Article35. van Kammen K, Boonstra AM, van der Woude LHV, Reinders-Messelink HA, den Otter R. Differences in muscle activity and temporal step parameters between Lokomat guided walking and treadmill walking in post-stroke hemiparetic patients and healthy walkers. J Neuroeng Rehabil. 2017; 14:32.
Article36. Semaan MB, Wallard L, Ruiz V, Gillet C, Leteneur S, Simoneau-Buessinger E. Is treadmill walking biomechanically comparable to overground walking? A systematic review. Gait Posture. 2022; 92:249–57.
Article37. Bowden MG, Balasubramanian CK, Neptune RR, Kautz SA. Anterior-posterior ground reaction forces as a measure of paretic leg contribution in hemiparetic walking. Stroke. 2006; 37:872–6.
Article38. Balasubramanian CK, Bowden MG, Neptune RR, Kautz SA. Relationship between step length asymmetry and walking performance in subjects with chronic hemiparesis. Arch Phys Med Rehabil. 2007; 88:43–9.
Article39. Awad LN, Binder-Macleod SA, Pohlig RT, Reisman DS. Paretic propulsion and trailing limb angle are key determinants of long-distance walking function after stroke. Neurorehabil Neural Repair. 2015; 29:499–508.
Article40. Varoqui D, Niu X, Mirbagheri MM. Ankle voluntary movement enhancement following robotic-assisted locomotor training in spinal cord injury. J Neuroeng Rehabil. 2014; 11:46.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Review of Robot-Assisted Gait Training in Stroke Patients
- Neuroplasticity Induced by Robot-assisted Gait Training in a Stroke Patient: A case report
- Feasibility and Usability of a Robot-Assisted Complex Upper and Lower Limb Rehabilitation System in Patients with Stroke: A Pilot Study
- Robot-assisted Therapy in Stroke Rehabilitation
- Effects of Robot-assisted Gait Therapy on Locomotor Recovery in Stroke Patients
