Ann Surg Treat Res.
2023 Jun;104(6):339-347. 10.4174/astr.2023.104.6.339.
Clinical outcomes of in situ graft reconstruction in treating infected abdominal aortic stent grafts following endovascular aortic aneurysm repair: a single-center experience
- Affiliations
-
- 1Division of Vascular Surgery, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Department of Acute Care Surgery, Korea University Guro Hospital, Seoul, Korea
- 3Armed Forces Trauma Center, Korean Armed Forces Capital Hospital, Seongnam, Korea
- KMID: 2542798
- DOI: http://doi.org/10.4174/astr.2023.104.6.339
Abstract
- Purpose
This study aimed to review our experience with the explantation of infected endovascular aneurysm repair (EVAR) grafts.
Methods
This single-center, retrospective, observational study analyzed the data of 12 consecutive patients who underwent infected aortic stent graft explantation following EVAR between January 1, 2010 and December 31, 2019, of which 11 underwent in situ graft reconstruction following graft removal. The presentation symptoms, infection route, original pathology of abdominal aortic aneurysms (AAA), graft materials, and clinical outcomes were analyzed.
Results
Six patients underwent total explantation, whereas 5 underwent removal of only the fabric portions. For in situ reconstructions, prosthetic grafts and banked allografts were used in 8 and 3 patients, respectively. Four mechanisms of graft infection were noted in 11 patients: 4 had bacteremia from systemic infections, 3 had persistent infections following EVAR of primary infected AAA, 3 had ascending infections from adjacent abscesses, and 1 had an aneurysm sac erosion resulting in an aortoenteric fistula. No infection-related postoperative complications or reinfections occurred during the mean 65.27-month (standard deviation, ±52.51) follow-up period. One patient died postoperatively because of the rupture of the proximal aortic wall pseudoaneurysm that had occurred during forceful bare stent removal.
Conclusion
Regardless of graft material, in situ graft reconstruction is safe for interposition in treating an infected aortic stent graft following EVAR. In our experience, the residual bare stent is no longer a risk factor for reinfection. Therefore, it is important not to injure the proximal aortic wall when removing the bare stent by force.
Figure
-
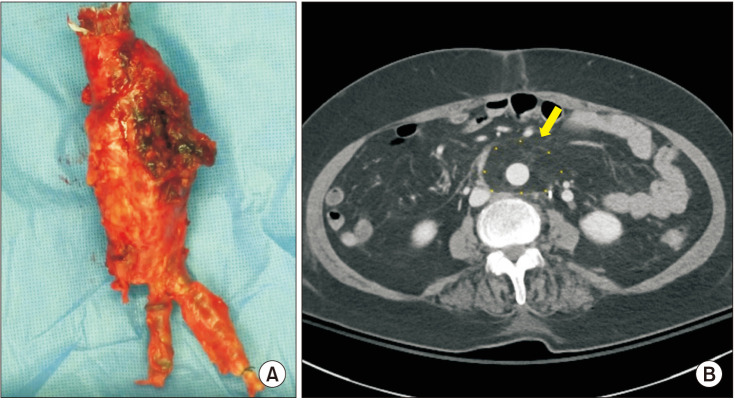
Fig. 1 (A) Surgical photo of the explanted stent graft (Gore Excluder, W. L. Gore & Associates, Inc.) of a patient who had persistent infection after endovascular aneurysm repair (EVAR) with an aortoduodenal fistula. The stent graft was removed completely. (B) Postoperative CT image of the patient who underwent in situ reconstruction after explantation of the infected EVAR graft, showing the patent Dacron graft with omental wrapping (yellow arrow).
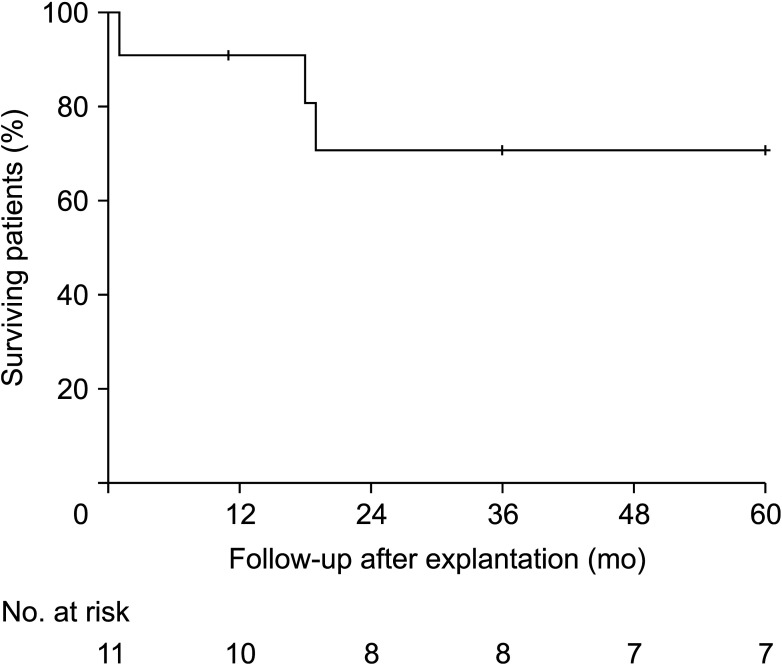
Fig. 2 The Kaplan-Meier estimate of overall 5-year survival rates among 11 patients with in situ reconstruction after explantation of infected stent grafts.
Reference
-
1. Chaikof EL, Dalman RL, Eskandari MK, Jackson BM, Lee WA, Mansour MA, et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg. 2018; 67:2–77. PMID: 29268916.2. Kim HO, Yim NY, Kim JK, Kang YJ, Lee BC. Endovascular aneurysm repair for abdominal aortic aneurysm: a comprehensive review. Korean J Radiol. 2019; 20:1247–1265. PMID: 31339013.3. Sharif MA, Lee B, Lau LL, Ellis PK, Collins AJ, Blair PH, et al. Prosthetic stent graft infection after endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2007; 46:442–448. PMID: 17826231.4. Heyer KS, Modi P, Morasch MD, Matsumura JS, Kibbe MR, Pearce WH, et al. Secondary infections of thoracic and abdominal aortic endografts. J Vasc Interv Radiol. 2009; 20:173–179. PMID: 19097807.5. Cernohorsky P, Reijnen MM, Tielliu IF, van Sterkenburg SM, van den Dungen JJ, Zeebregts CJ. The relevance of aortic endograft prosthetic infection. J Vasc Surg. 2011; 54:327–333. PMID: 21397443.6. Chung BH, Heo SH, Park YJ, Kim DI, Kim DK, Kim YW. Strategy to avoid open surgical conversion after endovascular aortic aneurysm repair for patients with infrarenal abdominal aortic aneurysm. Ann Surg Treat Res. 2020; 99:344–351. PMID: 33304862.7. Setacci C, Chisci E, Setacci F, Ercolini L, de Donato G, Troisi N, et al. How to diagnose and manage infected endografts after endovascular aneurysm repair. Aorta (Stamford). 2014; 2:255–264. PMID: 26798744.8. Wouthuyzen-Bakker M, van Oosten M, Bierman W, Winter R, Glaudemans A, Slart R, et al. Diagnosis and treatment of vascular graft and endograft infections: a structured clinical approach. Int J Infect Dis. 2023; 126:22–27. PMID: 36375692.9. Chakfé N, Diener H, Lejay A, Assadian O, Berard X, Caillon J, et al. Editor’s Choice: European Society for Vascular Surgery (ESVS) 2020 clinical practice guidelines on the management of vascular graft and endograft infections. Eur J Vasc Endovasc Surg. 2020; 59:339–384. PMID: 32035742.10. Kwon TW, Shin ES, Kim DK, Lee SO, Kim GE. Ruptured abdominal aortic aneurysms due to Salmonella, not of typhi species. Ann Vasc Surg. 2003; 17:464–467. PMID: 14670029.11. Han Y, Kwon TW, Park SJ, Jeong MJ, Choi K, Ko GY, et al. The results of in situ prosthetic graft replacement for infected aortic disease. World J Surg. 2018; 42:3035–3041. PMID: 29411065.12. Antonios VS, Noel AA, Steckelberg JM, Wilson WR, Mandrekar JN, Harmsen WS, et al. Prosthetic vascular graft infection: a risk factor analysis using a case-control study. J Infect. 2006; 53:49–55. PMID: 16310254.13. Wilson WR, Bower TC, Creager MA, Amin-Hanjani S, O’Gara PT, Lockhart PB, et al. Vascular graft infections, mycotic aneurysms, and endovascular infections: a scientific statement from the American Heart Association. Circulation. 2016; 134:e412–e460. PMID: 27737955.14. Luo CM, Chan CY, Chen YS, Wang SS, Chi NH, Wu IH. Long-term outcome of endovascular treatment for mycotic aortic aneurysm. Eur J Vasc Endovasc Surg. 2017; 54:464–471. PMID: 28826996.15. Kritpracha B, Premprabha D, Sungsiri J, Tantarattanapong W, Rookkapan S, Juntarapatin P. Endovascular therapy for infected aortic aneurysms. J Vasc Surg. 2011; 54:1259–1265. PMID: 21802238.16. Zaki M, Tawfick W, Alawy M, ElKassaby M, Hynes N, Sultan S. Secondary aortoduodenal fistula following endovascular repair of inflammatory abdominal aortic aneurysm due to Streptococcus anginosus infection: a case report and literature review. Int J Surg Case Rep. 2014; 5:710–713. PMID: 25201477.17. Burks JA Jr, Faries PL, Gravereaux EC, Hollier LH, Marin ML. Endovascular repair of bleeding aortoenteric fistulas: a 5-year experience. J Vasc Surg. 2001; 34:1055–1059. PMID: 11743560.18. Argyriou C, Georgiadis GS, Lazarides MK, Georgakarakos E, Antoniou GA. Endograft infection after endovascular abdominal aortic aneurysm repair: a systematic review and meta-analysis. J Endovasc Ther. 2017; 24:688–697. PMID: 28756719.19. Kwon TW, Kim HK, Moon KM, Cho YP, Park SJ. In situ polytetrafluoroethylene graft bypass for primary infected aneurysm of the infrarenal abdominal aorta. World J Surg. 2010; 34:1689–1695. PMID: 20238215.20. Park SJ, Kim MN, Kwon TW. Infected abdominal aortic aneurysm caused by Brucella abortus: a case report. J Vasc Surg. 2007; 46:1277–1279. PMID: 18155006.21. Koning OH, Hinnen JW, van Baalen JM. Technique for safe removal of an aortic endograft with suprarenal fixation. J Vasc Surg. 2006; 43:855–857. PMID: 16616252.22. Filis KA, Galyfos G, Sigala F, Tsioufis K, Tsagos I, Karantzikos G, et al. Proximal aortic neck progression: before and after abdominal aortic aneurysm treatment. Front Surg. 2017; 4:23. PMID: 28523269.23. Popplewell MA, Garnham AW, Hobbs SD. A new technique to explant an infected aortic endograft. J Vasc Surg. 2015; 62:512–514. PMID: 25937607.24. Boyle E, McHugh SM, Elmallah A, Lynch M, McGuire D, Ahmed Z, et al. Explant of aortic stent grafts following endovascular aneurysm repair. Vascular. 2019; 27:487–494. PMID: 30880610.25. Shukuzawa K, Ohki T, Maeda K, Kanaoka Y. Risk factors and treatment outcomes for stent graft infection after endovascular aortic aneurysm repair. J Vasc Surg. 2019; 70:181–192. PMID: 30583901.26. Armstrong PA, Back MR, Wilson JS, Shames ML, Johnson BL, Bandyk DF. Improved outcomes in the recent management of secondary aortoenteric fistula. J Vasc Surg. 2005; 42:660–666. PMID: 16242551.27. Ali A, Bahia SS, Ali T. Cadaveric aorta implantation for aortic graft infection. Int J Surg Case Rep. 2016; 25:120–127. PMID: 27351624.28. Langenskiöld M, Persson SE, Daryapeyma A, Gillgren P, Hallin A, Hultgren R, et al. Deep femoral vein reconstruction for abdominal aortic graft infections is associated with low aneurysm related mortality and a high rate of permanent discontinuation of antimicrobial treatment. Eur J Vasc Endovasc Surg. 2021; 62:927–934. PMID: 34686449.29. Filiberto AC, Scali ST, Patterson S, Neal D, Elder CT, Shah SK, et al. Treatment and outcomes of aortic graft infections using a decision algorithm. Ann Vasc Surg. 2021; 76:254–268. PMID: 34182116.30. Yamanaka K, Omura A, Nomura Y, Miyahara S, Shirasaka T, Sakamoto T, et al. Surgical strategy for aorta-related infection. Eur J Cardiothorac Surg. 2014; 46:974–980. PMID: 24699204.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Repair of Thoracic Aortic Aneurysm Using a Custom-made Fenestrated Stent Graft to Preserve the Left Subclavian Artery
- Endovascular Stent-Graft Placement and Secondary Intervention for Abdominal Aortic Aneurysm in a Patient who had a Previously Inserted Iliac Stent
- Aortic Endograft Infection: Diagnosis and Management
- Endovascular Treatment of Abdominal Aortic Aneurysm
- Endovascular Repair of a Juxtarenal Abdominal Aortic Aneurysm Using a Chimney Graft
