Successful removal of remnant cystic duct stump stone using single-operator cholangioscopy-guided electrohydraulic lithotripsy: two case reports
- Affiliations
-
- 1Department of Gastroenterology, Dankook University Hospital, Dankook University College of Medicine, Cheonan, Korea
- KMID: 2542465
- DOI: http://doi.org/10.5946/ce.2021.273
Abstract
- Cholecystectomy is the best method for treating gallstone diseases. However, 10%–30% of patients who undergo a cholecystectomy continue to complain of upper abdominal pain, dyspepsia, or jaundice—this is referred to as postcholecystectomy syndrome. Cystic duct stump stones are a troublesome cause of postcholecystectomy syndrome. Conventionally, surgery is mainly performed to remove cystic duct stump stones. However, repeated surgery can cause complications, such as postoperative bleeding, biliary injury, and wound infection. As an alternative method of surgery, endoscopic retrograde cholangiopancreatography is sometimes used to remove cystic duct stump stones, although the success rate is not high due to technical difficulties. Recently, peroral cholangioscopy, which can directly observe the bile duct, has been suggested as an alternative method. We report two cases in which a cystic duct stump stone was successfully removed via a single-operator cholangioscopy, after failure with an endoscopic retrograde cholangiopancreatography.
Keyword
Figure
-
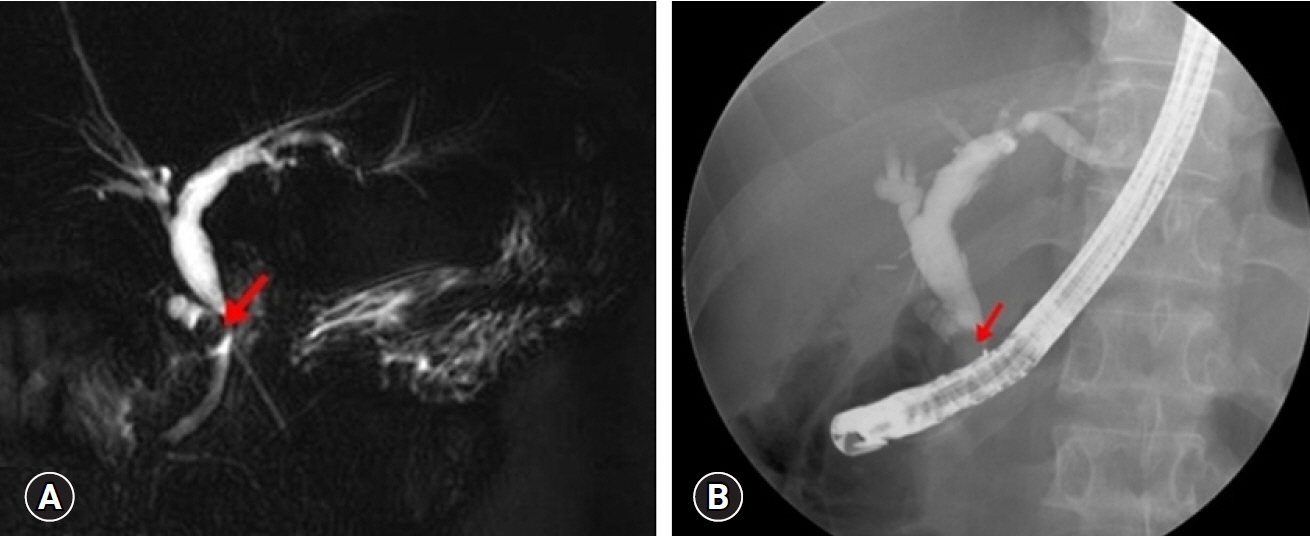
Fig. 1. Magnetic resonance cholangiopancreatography and endoscopic retrograde cholangiopancreatography findings. (A) An 8-mm-sized filling defect (arrow) in the remnant cystic duct compressing the proximal common bile duct and dilating the remnant cystic duct stump. (B) The impacted cystic duct stone (arrow) is observed on ERCP.

Fig. 2. Removal of the cystic duct stump stone by single-operator cholangioscopy (SOC) with electrohydraulic lithotripsy (EHL) and follow-up endoscopic retrograde cholangiopancreatography (ERCP) findings after endoscopic treatment. (A) The impacted stone (arrow) is observed on the cystic duct stump by SOC. (B) After using EHL, the stone was removed. (C) There is no evidence of the cystic duct stump stone on ERCP.
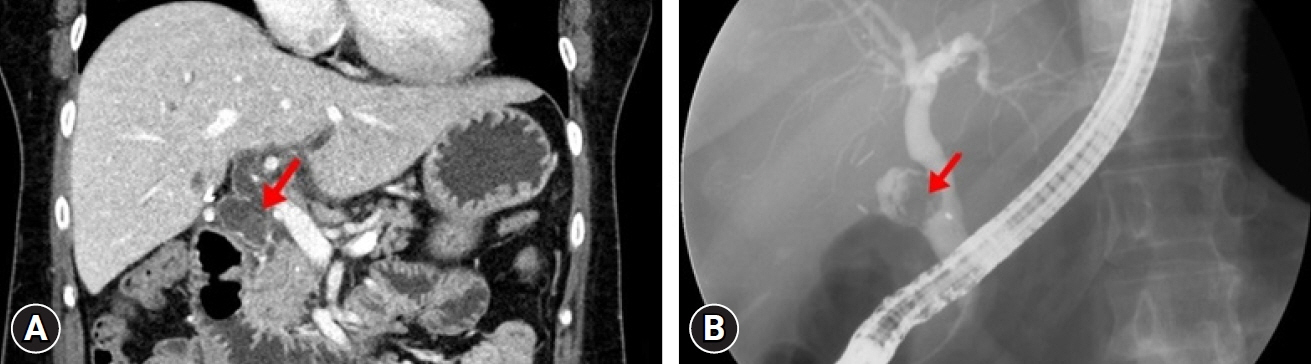
Fig. 3. Abdominopelvic computed tomography (CT) and endoscopic retrograde cholangiopancreatography (ERCP) findings. (A) Remnant cystic duct dilatation (arrow) with common bile duct dilatation is observed on CT. (B) The stone is impacted in the cystic duct stump (arrow).
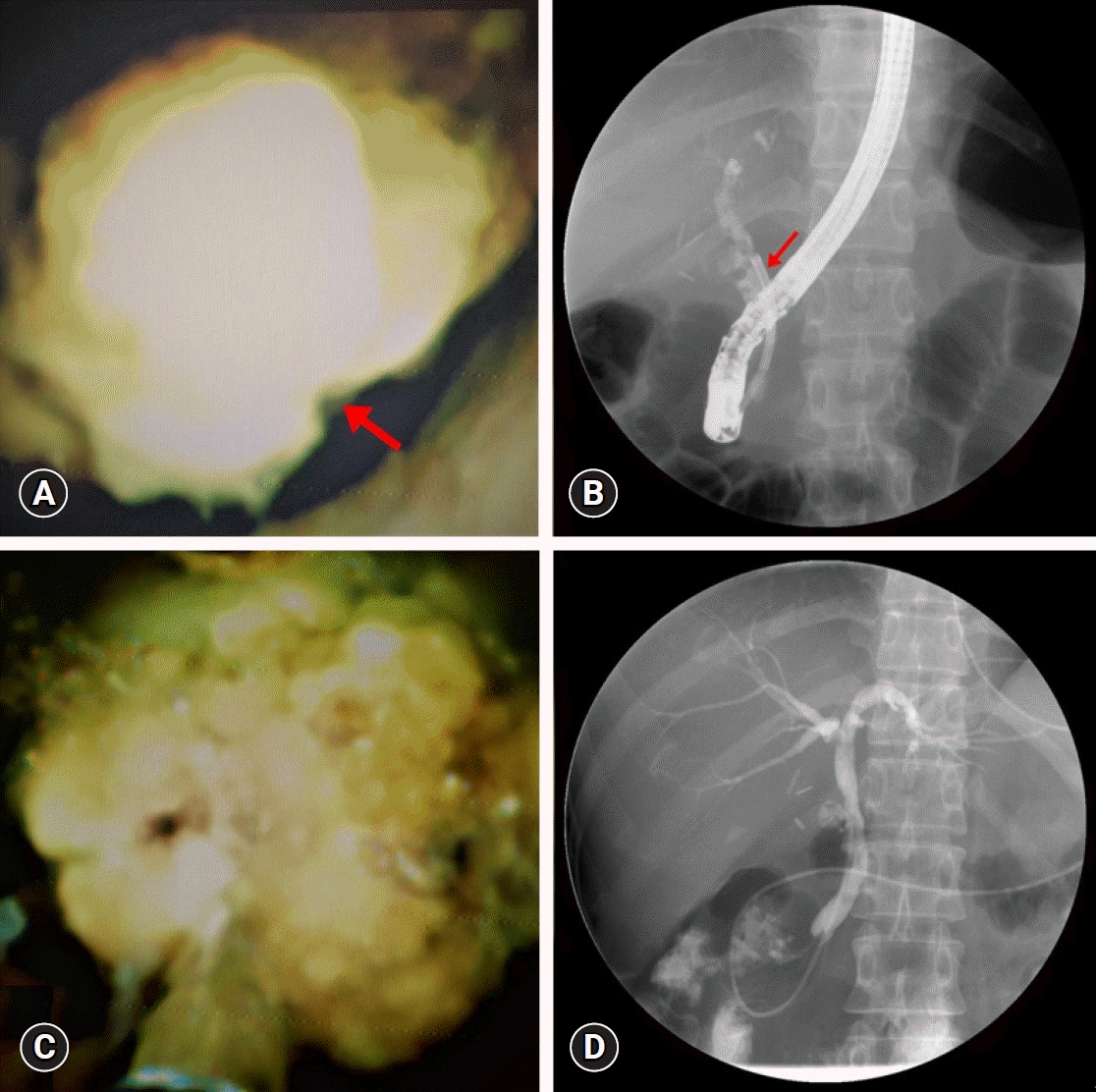
Fig. 4. Removal of cystic duct stump stone by single-operator cholangioscopy (SOC) with electrohydraulic lithotripsy (EHL) and follow-up endoscopic retrograde cholangiopancreatography (ERCP) findings after endoscopic treatment. (A) The impacted stone (arrow) is observed on the cystic duct stump by SOC. (B) Fluoroscopic image of SOC (arrow) targeting the impacted cystic duct stone. (C) The stone was fragmented using EHL. (D) There is no evidence of the cystic duct stump stone on ERCP.
Reference
-
1. El Nakeeb A, Ezzat H, Askar W, et al. Management of residual gallbladder and cystic duct stump stone after cholecystectomy: a retrospective study. Egyptian J Surg. 2016; 35:391–397.2. Schofer JM. Biliary causes of postcholecystectomy syndrome. J Emerg Med. 2010; 39:406–410.3. Walsh RM, Ponsky JL, Dumot J. Retained gallbladder/cystic duct remnant calculi as a cause of postcholecystectomy pain. Surg Endosc. 2002; 16:981–984.4. Palanivelu C, Rangarajan M, Jategaonkar PA, et al. Laparoscopic management of remnant cystic duct calculi: a retrospective study. Ann R Coll Surg Engl. 2009; 91:25–29.5. Mageed SA, Omar MA, Redwan AA. Remnant gallbladder and cystic duct stump stone after cholecystectomy: tertiary multicenter experience. Int Surg J. 2018; 5:3478–3483.6. Issa H, Bseiso B, Almousa F, et al. Successful treatment of Mirizzi’s syndrome using SpyGlass guided laser lithotripsy. Gastroenterology Res. 2012; 5:162–166.7. Shirah BH, Shirah HA, Zafar SH, et al. Clinical patterns of postcholecystectomy syndrome. Ann Hepatobiliary Pancreat Surg. 2018; 22:52–57.8. Rieger R, Wayand W. Gallbladder remnant after laparoscopic cholecystectomy. Surg Endosc. 1995; 9:844.9. Rozsos I, Magyarodi Z, Orban P. Cystic duct syndrome and minimally invasive surgery. Orv Hetil. 1997; 138:2397–2401.10. Parmar AK, Khandelwal RG, Mathew MJ, et al. Laparoscopic completion cholecystectomy: a retrospective study of 40 cases. Asian J Endosc Surg. 2013; 6:96–99.11. Kim JY, Kim KW, Ahn CS, et al. Spectrum of biliary and nonbiliary complications after laparoscopic cholecystectomy: radiologic findings. AJR Am J Roentgenol. 2008; 191:783–789.12. Rozsos I, Magyaródi Z, Orbán P. The removal of cystic duct and gallbladder remnant by microlaparotomy. Acta Chir Hung. 1997; 36:297–298.13. Kar A, Gulati S, Mohammed S, et al. Surgical management of cystic duct stump stone or gallbladder remnant stone. Indian J Surg. 2018; 80:284–287.14. England RE, Martin DF. Endoscopic management of Mirizzi’s syndrome. Gut. 1997; 40:272–276.15. Ghersi S, Fuccio L, Bassi M, et al. Current status of peroral cholangioscopy in biliary tract diseases. World J Gastrointest Endosc. 2015; 7:510–517.16. Franzini TA, Moura RN, de Moura EG. Advances in therapeutic cholangioscopy. Gastroenterol Res Pract. 2016; 2016:5249152.17. Seelhoff A, Schumacher B, Neuhaus H. Single operator peroral cholangioscopic guided therapy of bile duct stones. J Hepatobiliary Pancreat Sci. 2011; 18:346–349.18. Sandha J, van Zanten SV, Sandha G. The safety and efficacy of single-operator cholangioscopy in the treatment of difficult common bile duct stones after failed conventional ERCP. J Can Assoc Gastroenterol. 2018; 1:181–190.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Minimally Invasive Approach Using Digital Single-Operator Peroral Cholangioscopy-Guided Electrohydraulic Lithotripsy and Endoscopic Nasogallbladder Drainage for the Management of High-Grade Mirizzi Syndrome
- Single-operator Cholangioscopy Guided Lithotripsy
- Recent advances in the management of difficult bile-duct stones: a focus on single-operator cholangioscopy-guided lithotripsy
- Successful Endoscopic Treatment of Difficult Common Bile Duct Stones Using Various Interventional Techniques: A Case Report
- Utility of Direct Peroral Cholangioscopy Using a Multibending Ultraslim Endoscope for Difficult Common Bile Duct Stones
