Clin Exp Otorhinolaryngol.
2023 May;16(2):177-183. 10.21053/ceo.2023.00031.
The Clinical Features and Risk Factors of Subglottic Cysts in Children: A Clinical Experience Using the Spontaneous Respiration Technique
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Hallym University Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University Hospital, Seoul, Korea
- 3Interdisciplinary Program in Stem Cell Biology, Seoul National University, Seoul, Korea
- 4Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University College of Medicine, Seoul, Korea
- 5Cancer Research Institute , Seoul National University, Seoul, Korea
- 6Sensory Organ Research Institute, Seoul National University Medical Research Center, Seoul, Korea
- KMID: 2542359
- DOI: http://doi.org/10.21053/ceo.2023.00031
Abstract
Objectives
. Subglottic cysts (SGCs) are a rare cause of respiratory distress resulting from upper airway obstruction in infants and young children. Risk factors other than prematurity with a history of endotracheal intubation have not yet been well elucidated. Therefore, we aimed to describe the clinical features and analyze the risk factors of SGCs.
Methods
. We conducted a retrospective review of medical records of pediatric patients who underwent marsupialization for SGCs between January 2017 and March 2022. These records were then compared with those of controls with a history of neonatal intubation, with a case-to-control ratio of 1:3.
Results
. Eleven patients (eight boys and three girls) diagnosed with SGCs and 33 control patients (26 boys and seven girls) were included. All patients had a history of premature birth and neonatal intubation. Symptoms of SGCs appeared at a mean age of 8.2 months (range, 1–14 months) after extubation. The mean duration of intubation was 21.5 days (range, 2–90 days), and the intubation period was longer in patients with SGCs than in controls (21.5±24.8 days vs. 5.3±7.1 days; P<0.001). Furthermore, gestational age (28.3±4.2 weeks vs. 33.8±4.4 weeks; P=0.001) and birth weight (1,134.1±515.1 g vs. 2,178.2±910.1 g; P=0.001) were significantly lower in patients with SGCs than in controls. Multivariable analysis identified the intubation period as an independent risk factor.
Conclusion
. This study showed that gestational age, birth weight, and the intubation period were significantly associated with the development of SGCs. Pediatric patients presenting with progressive dyspnea who have the corresponding risk factors should undergo early laryngoscopy for the differential diagnosis of SGC.
Keyword
Figure
-
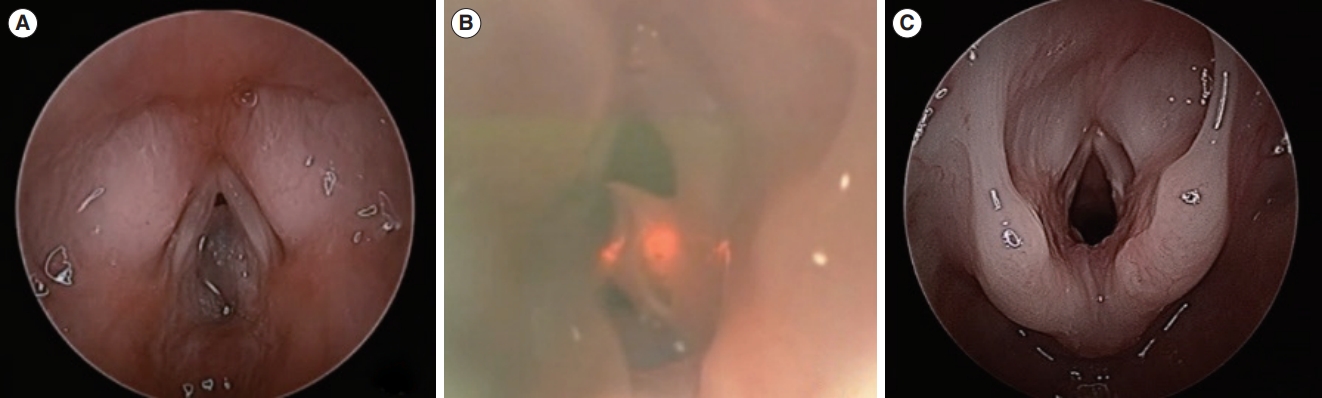
Fig. 1. (A) A bilateral subglottic cyst with transparent, thin capsules that obstruct more than 75% of the subglottis. (B) Marsupialization of subglottic cysts using a CO2 laser with the STRIVE Hi anesthesia technique. (C) Postoperative view after complete marsupialization. STRIVE Hi, SponTaneous Respiration using IntraVEnous anesthesia and Hi-flow nasal oxygen.
Reference
-
1. Wigger HJ, Tang P. Fatal laryngeal obstruction by iatrogenic subglottic cyst. J Pediatr. 1968; Jun. 72(6):815–20.
Article2. Gould SJ, Young M. Subglottic ulceration and healing following endotracheal intubation in the neonate: a morphometric study. Ann Otol Rhinol Laryngol. 1992; Oct. 101(10):815–20.
Article3. Bowles PF, Reading J, Albert D, Nash R. Subglottic cysts: the Great Ormond Street experience in 105 patients. Eur Arch Otorhinolaryngol. 2021; Jun. 278(6):2137–41.
Article4. Aksoy EA, Elsurer C, Serin GM, Unal OF. Evaluation of pediatric subglottic cysts. Int J Pediatr Otorhinolaryngol. 2012; Feb. 76(2):240–3.
Article5. Johnson LB, Rutter MJ, Shott SR, Cotton RT. Acquired subglottic cysts in preterm infants. J Otolaryngol. 2005; Apr. 34(2):75–8.
Article6. Lim J, Hellier W, Harcourt J, Leighton S, Albert D. Subglottic cysts: the Great Ormond Street experience. Int J Pediatr Otorhinolaryngol. 2003; May. 67(5):461–5.
Article7. Jaryszak EM, Collins WO. Microdebrider resection of bilateral subglottic cysts in a pre-term infant: a novel approach. Int J Pediatr Otorhinolaryngol. 2009; Jan. 73(1):139–42.
Article8. Halimi C, Nevoux J, Denoyelle F, Garabedian EN, Leboulanger N. Acquired subglottic cysts: management and long term outcome. Int J Pediatr Otorhinolaryngol. 2012; Apr. 76(4):589–92.
Article9. Soloperto D, Spinnato F, Di Gioia S, Di Maro F, Pinter P, Bisceglia A, et al. Acquired subglottic cysts in children: a rare and challenging clinical entity: a systematic review. Int J Pediatr Otorhinolaryngol. 2021; Jan. 140:110523.
Article10. Smith SP, Berkowitz RG, Phelan PD. Acquired subglottic cysts in infancy. Arch Otolaryngol Head Neck Surg. 1994; Sep. 120(9):921–4.
Article11. Weisberger EC, Emhardt JD. Apneic anesthesia with intermittent ventilation for microsurgery of the upper airway. Laryngoscope. 1996; Sep. 106(9 Pt 1):1099–102.
Article12. Booth AW, Vidhani K, Lee PK, Thomsett CM. SponTaneous Respiration using IntraVEnous anaesthesia and Hi-flow nasal oxygen (STRIVE Hi) maintains oxygenation and airway patency during management of the obstructed airway: an observational study. Br J Anaesth. 2017; Mar. 118(3):444–51.
Article13. Ji JY, Kim EH, Lee JH, Jang YE, Kim HS, Kwon SK. Pediatric airway surgery under spontaneous respiration using high-flow nasal oxygen. Int J Pediatr Otorhinolaryngol. 2020; Jul. 134:110042.
Article14. Cha H, Lee DY, Kim EH, Lee JH, Jang YE, Kim HS, et al. Feasibility of surgical treatment for laryngomalacia using the spontaneous respiration technique. Clin Exp Otorhinolaryngol. 2021; Nov. 14(4):414–23.
Article15. Knol MJ, Vandenbroucke JP, Scott P, Egger M. What do case-control studies estimate?: survey of methods and assumptions in published case-control research. Am J Epidemiol. 2008; Nov. 168(9):1073–81.
Article16. Watson GJ, Malik TH, Khan NA, Sheehan PZ, Rothera MP. Acquired paediatric subglottic cysts: a series from Manchester. Int J Pediatr Otorhinolaryngol. 2007; Apr. 71(4):533–8.
Article17. Bruce IA, Rothera MP. Upper airway obstruction in children. Paediatr Anaesth. 2009; Jul. 19 Suppl 1:88–99.
Article18. Richardson MA, Winford TW, Norris BK, Reed JM. Management of pediatric subglottic cysts using the Bugbee fulgurating electrode. JAMA Otolaryngol Head Neck Surg. 2014; Feb. 140(2):164–8.
Article19. Reed JM, Myer CM 3rd. Radiographic evaluation of a subglottic cyst in an infant. Am J Otolaryngol. 1995; Sep-Oct. 16(5):329–30.
Article20. Agada FO, Bell J, Knight L. Subglottic cysts in children: a 10-year review. Int J Pediatr Otorhinolaryngol. 2006; Aug. 70(8):1485–8.
Article21. Ransom ER, Antunes MB, Smith LP, Jacobs IN. Microdebrider resection of acquired subglottic cysts: case series and review of the literature. Int J Pediatr Otorhinolaryngol. 2009; Dec. 73(12):1833–6.
Article22. Steehler MK, Groblewski JC, Milmoe GJ, Harley EH. Management of subglottic cysts with Mitomycin-C: a case series and literature review. Int J Pediatr Otorhinolaryngol. 2011; Mar. 75(3):360–3.23. Jaquet Y, Monnier P, Van Melle G, Ravussin P, Spahn DR, CholletRivier M. Complications of different ventilation strategies in endoscopic laryngeal surgery: a 10-year review. Anesthesiology. 2006; Jan. 104(1):52–9.24. Riva T, Theiler L, Jaquet Y, Giger R, Nisa L. Early experience with high-flow nasal oxygen therapy (HFNOT) in pediatric endoscopic airway surgery. Int J Pediatr Otorhinolaryngol. 2018; May. 108:151–4.
Article25. Toriumi DM, Miller DR, Holinger LD. Acquired subglottic cysts in premature infants. Int J Pediatr Otorhinolaryngol. 1987; Dec. 14(2-3):151–60.
Article26. Smith JD, Cotton R, Meyer CM 3rd. Subglottic cysts in the premature infant. Arch Otolaryngol Head Neck Surg. 1990; Apr. 116(4):479–82.
Article27. Tierney PA, Francis I, Morrison GA. Acquired subglottic cysts in the low birth weight, pre-term infant. J Laryngol Otol. 1997; May. 111(5):478–81.
Article28. Vo DN. Anesthesia for patients with subglottic cysts. Clin Case Rep. 2016; Jan. 4(2):209–11.
Article29. Unsaler S, Gokler O, Altuntas O, Meris Hafiz A, Unal OF. Subglottic cysts in preterm infants: superficially located cysts versus deeply buried cysts in the mucosa. Eur Arch Otorhinolaryngol. 2022; Mar. 279(3):1391–6.
Article30. Rasche RF, Kuhns LR. Histopathologic changes in airway mucosa of infants after endotracheal intubation. Pediatrics. 1972; Oct. 50(4):632–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Expandable Metallic Stent in the Treatment of Subglottic Tracheal Stenosis: Report of Long-term Failure in 4 Cases
- An infant with subglottic cysts presenting as abruptly-progressed stridor and respiratory distress 2 months after extubation
- Clinical Features of Risk factors and Regression of Retinopathy of Prematurity
- Etiologies and Clinical Courses of Stridor with Respiratory Distress of Non-infectious Origin in Infants and Children
- Early recognition of high risk factors of acute abdominal pain in children
