Acute Crit Care.
2022 Nov;37(4):483-490. 10.4266/acc.2022.01291.
Target temperature management in traumatic brain injury with a focus on adverse events, recognition, and prevention
- Affiliations
-
- 1Department of Neurosurgery, Bucheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2540136
- DOI: http://doi.org/10.4266/acc.2022.01291
Abstract
- Traumatic brain injury (TBI) is a critical cause of disability and death worldwide. Many studies have been conducted aimed at achieving favorable neurologic outcomes by reducing secondary brain injury in TBI patients. However, ground-breaking outcomes are still insufficient so far. Because mild-to-moderate hypothermia (32°C–35°C) has been confirmed to help neurological recovery for recovered patients after circulatory arrest, it has been recognized as a major neuroprotective treatment plan for TBI patients. Thereafter, many clinical studies about the effect of therapeutic hypothermia (TH) on severe TBI have been conducted. However, efficacy and safety have not been demonstrated in many large-scale randomized controlled studies. Rather, some studies have demonstrated an increase in mortality rate due to complications such as pneumonia, so it is not highly recommended for severe TBI patients. Recently, some studies have shown results suggesting TH may help reperfusion/ischemic injury prevention after surgery in the case of mass lesions, such as acute subdural hematoma, and it has also been shown to be effective in intracranial pressure control. In conclusion, TH is still at the center of neuroprotective therapeutic studies regarding TBI. If proper measures can be taken to mitigate the many adverse events that may occur during the course of treatment, more positive efficacy can be confirmed. In this review, we look into adverse events that may occur during the process of the induction, maintenance, and rewarming of targeted temperature management and consider ways to prevent and address them.
Keyword
Figure
-

Figure 1. Shivering management [19,27]. Continuous electroencephalogram monitoring may be considered for early detection of nonconvulsive status epilepticus for Stages 2 and 3.
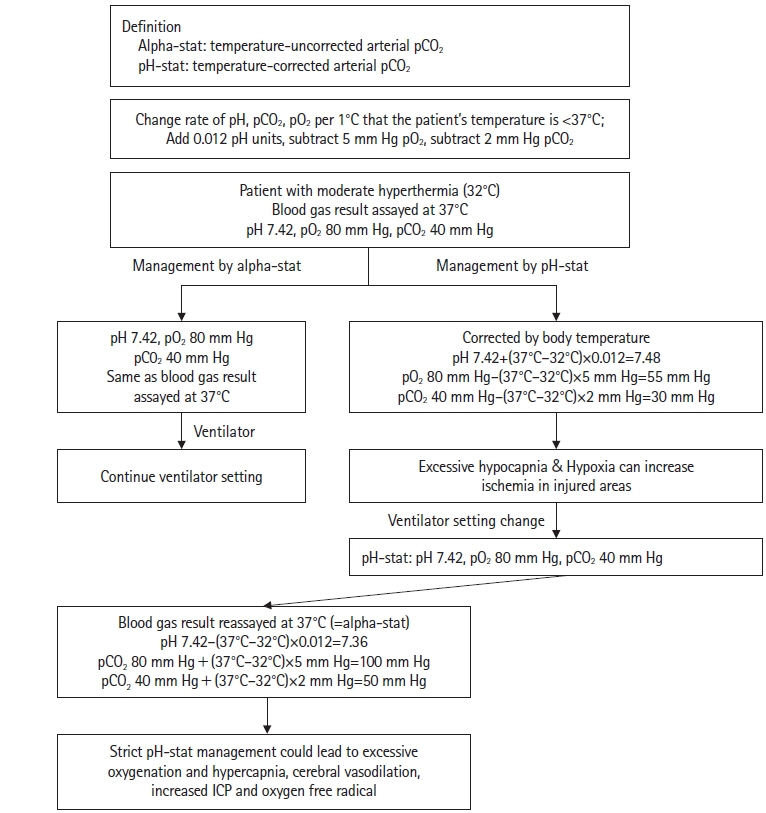
Figure 2. Different management plans according to alpha-stat and pH-stat. ICP: intracranial pressure.
Reference
-
1. Maekawa T, Yamashita S, Nagao S, Hayashi N, Ohashi Y, Brain-Hypothermia Study Group. Prolonged mild therapeutic hypothermia versus fever control with tight hemodynamic monitoring and slow rewarming in patients with severe traumatic brain injury: a randomized controlled trial. J Neurotrauma. 2015; 32:422–9.
Article2. Cooper DJ, Nichol AD, Bailey M, Bernard S, Cameron PA, Pili-Floury S, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR Randomized Clinical Trial. JAMA. 2018; 320:2211–20.
Article3. O’Leary R, Hutchinson PJ, Menon D. Hypothermia for intracranial hypertension after traumatic brain injury. N Engl J Med. 2016; 374:1383–4.
Article4. Clifton GL, Coffey CS, Fourwinds S, Zygun D, Valadka A, Smith KR Jr, et al. Early induction of hypothermia for evacuated intracranial hematomas: a post hoc analysis of two clinical trials. J Neurosurg. 2012; 117:714–20.
Article5. Carney N, Totten AM, O’Reilly C, Ullman JS, Hawryluk GW, Bell MJ, et al. Guidelines for the management of severe traumatic brain injury, fourth edition. Neurosurgery. 2017; 80:6–15.
Article6. Rehman T, deBoisblanc BP. Persistent fever in the ICU. Chest. 2014; 145:158–65.
Article7. Diringer MN, Reaven NL, Funk SE, Uman GC. Elevated body temperature independently contributes to increased length of stay in neurologic intensive care unit patients. Crit Care Med. 2004; 32:1489–95.
Article8. Kilpatrick MM, Lowry DW, Firlik AD, Yonas H, Marion DW. Hyperthermia in the neurosurgical intensive care unit. Neurosurgery. 2000; 47:850–6.
Article9. Lascarrou JB, Merdji H, Le Gouge A, Colin G, Grillet G, Girardie P, et al. Targeted temperature management for cardiac arrest with nonshockable rhythm. N Engl J Med. 2019; 381:2327–37.
Article10. Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002; 346:557–63.
Article11. Berg KM, Soar J, Andersen LW, Böttiger BW, Cacciola S, Callaway CW, et al. Adult advanced life support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation. 2020; 142(16_suppl_1):S92–139.12. Nolan JP, Sandroni C, Böttiger BW, Cariou A, Cronberg T, Friberg H, et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care. Intensive Care Med. 2021; 47:369–421.
Article13. Panchal AR, Bartos JA, Cabañas JG, Donnino MW, Drennan IR, Hirsch KG, et al. Part 3: adult basic and advanced life support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020; 142(16_suppl_2):S366–468.14. Choi HA, Badjatia N, Mayer SA. Hypothermia for acute brain injury: mechanisms and practical aspects. Nat Rev Neurol. 2012; 8:214–22.
Article15. Madden LK, Hill M, May TL, Human T, Guanci MM, Jacobi J, et al. The implementation of targeted temperature management: an evidence-based guideline from the Neurocritical Care Society. Neurocrit Care. 2017; 27:468–87.
Article16. Staykov D, Wagner I, Volbers B, Doerfler A, Schwab S, Kollmar R. Mild prolonged hypothermia for large intracerebral hemorrhage. Neurocrit Care. 2013; 18:178–83.
Article17. Brott T, Bogousslavsky J. Treatment of acute ischemic stroke. N Engl J Med. 2000; 343:710–22.
Article18. Badjatia N. Hypothermia in neurocritical care. Neurosurg Clin N Am. 2013; 24:457–67.
Article19. Polderman KH, Herold I. Therapeutic hypothermia and controlled normothermia in the intensive care unit: practical considerations, side effects, and cooling methods. Crit Care Med. 2009; 37:1101–20.
Article20. Cariou A, Payen JF, Asehnoune K, Audibert G, Botte A, Brissaud O, et al. Targeted temperature management in the ICU: guidelines from a French expert panel. Ann Intensive Care. 2017; 7:70.
Article21. Schell-Chaple HM, Liu KD, Matthay MA, Puntillo KA. Rectal and bladder temperatures vs forehead core temperatures measured with SpotOn monitoring system. Am J Crit Care. 2018; 27:43–50.
Article22. De Witte J, Sessler DI. Perioperative shivering: physiology and pharmacology. Anesthesiology. 2002; 96:467–84.23. Badjatia N, Strongilis E, Gordon E, Prescutti M, Fernandez L, Fernandez A, et al. Metabolic impact of shivering during therapeutic temperature modulation: the Bedside Shivering Assessment Scale. Stroke. 2008; 39:3242–7.
Article24. Rittenberger JC, Polderman KH, Smith WS, Weingart SD. Emergency neurological life support: resuscitation following cardiac arrest. Neurocrit Care. 2012; 17 Suppl 1:S21–8.
Article25. Polderman KH. Mechanisms of action, physiological effects, and complications of hypothermia. Crit Care Med. 2009; 37(7 Suppl):S186–202.
Article26. Mangat HS, Wu X, Gerber LM, Schwarz JT, Fakhar M, Murthy SB, et al. Hypertonic saline is superior to mannitol for the combined effect on intracranial pressure and cerebral perfusion pressure burdens in patients with severe traumatic brain injury. Neurosurgery. 2020; 86:221–30.
Article27. Kuroda Y, Kawakita K. Targeted temperature management for postcardiac arrest syndrome. J Neurocrit Care. 2020; 13:1–18.
Article28. Gagnon DJ, Nielsen N, Fraser GL, Riker RR, Dziodzio J, Sunde K, et al. Prophylactic antibiotics are associated with a lower incidence of pneumonia in cardiac arrest survivors treated with targeted temperature management. Resuscitation. 2015; 92:154–9.
Article29. Rohrer MJ, Natale AM. Effect of hypothermia on the coagulation cascade. Crit Care Med. 1992; 20:1402–5.
Article30. Crochemore T, Piza FM, Rodrigues RD, Guerra JC, Ferraz LJ, Corrêa TD. A new era of thromboelastometry. Einstein (Sao Paulo). 2017; 15:380–5.
Article31. Bruining HA, Boelhouwer RU. Acute transient hypokalemia and body temperature. Lancet. 1982; 2:1283–4.32. Polderman KH, Peerdeman SM, Girbes AR. Hypophosphatemia and hypomagnesemia induced by cooling in patients with severe head injury. J Neurosurg. 2001; 94:697–705.
Article33. Erecinska M, Thoresen M, Silver IA. Effects of hypothermia on energy metabolism in Mammalian central nervous system. J Cereb Blood Flow Metab. 2003; 23:513–30.
Article34. van der Worp HB, Macleod MR, Kollmar R, European Stroke Research Network for Hypothermia (EuroHYP). Therapeutic hypothermia for acute ischemic stroke: ready to start large randomized trials? J Cereb Blood Flow Metab. 2010; 30:1079–93.
Article35. Vespa PM, Nuwer MR, Nenov V, Ronne-Engstrom E, Hovda DA, Bergsneider M, et al. Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring. J Neurosurg. 1999; 91:750–60.
Article36. Auer RN. Non-pharmacologic (physiologic) neuroprotection in the treatment of brain ischemia. Ann N Y Acad Sci. 2001; 939:271–82.
Article37. Kaneko T, Fujita M, Yamashita S, Oda Y, Suehiro E, Dohi K, et al. Slow rewarming improved the neurological outcomes of prolonged mild therapeutic hypothermia in patients with severe traumatic brain injury and an evacuated hematoma. Sci Rep. 2018; 8:11630.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anesthetic management of the traumatic brain injury patients undergoing non-neurosurgery
- Targeted temperature management in brain edema
- Controversies in Acute Care of Patients with Severe Traumatic Brain Injury
- Metabolism of Valproate in Traumatic Brain Injury Patients
- Traumatic Brain injury and Sleep Disorder
