Association Between Receipt of General Anesthesia During Childhood and Attention Deficit Hyperactive Disorder and Neurodevelopment
- Affiliations
-
- 1Department of Pediatrics, CHA Gangnam Medical Center, CHA University School of Medicine, Seoul, Korea
- 2Department of Computer Science and Engineering, Sungkyunkwan University, Suwon, Korea
- 3Department of Precision Medicine, Sungkyunkwan University School of Medicine, Suwon, Korea
- 4Department of Pediatrics, Hallym University Kangnam Sacred Heart Hospital, Seoul, Korea
- 5Department of Pediatrics, Hallym University Kangdong Sacred Heart Hospital, Seoul, Korea
- 6Department of Pediatrics, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea
- KMID: 2539491
- DOI: http://doi.org/10.3346/jkms.2023.38.e42
Abstract
- Background
There are inconsistent reports regarding the association between general anesthesia and adverse neurodevelopmental and behavioral disorders in children.
Methods
This nationwide administrative cohort study included children born in Korea between 2008 and 2009, and followed until December 31, 2017. The cohort included 93,717 participants who received general anesthesia with endotracheal intubation (ETI) who were matched to unexposed subjects in a 1:1 ratio. General anesthesia was defined by National Health Insurance Service treatment codes with intratracheal anesthesia, and the index date was the first event of general anesthesia. The primary outcome was attention deficit hyperactive disorder (ADHD), which was defined as at least a principal diagnosis of 10th revision of the International Classification of Diseases code F90.X after the age of 72 months. Neurodevelopment, which was assessed using a developmental screening test (Korean-Ages and Stages Questionnaire [K-ASQ]), was a secondary outcome. The K-ASQ is performed annually from 1 to 6 years of age and consists of 5 domains. The association between general anesthesia and ADHD was estimated using a Cox hazard model, and its association with neurodevelopment was estimated using a generalized estimation equation, with control for multiple risk factors beyond 1 year after the index date.
Results
The median age at the index date was 3.8 (95% confidence interval [CI], 1.7–5.8) years, and there were 57,625 (61.5%) men. During a mean follow-up period of 5 years, the incidence rate of ADHD was 42.6 and 27.7 per 10,000 person-years (PY) in the exposed and unexposed groups, respectively (absolute rate difference 14.9 [95% CI, 12.5–17.3] per 10,000 PY). Compared to the unexposed group, the exposed group had an increased risk of ADHD (adjusted hazard ratio, 1.41 [95% CI, 1.30–1.52]). In addition, a longer duration of anesthesia with ETI and more general anesthesia procedures with ETI were associated with greater risk of ADHD. General anesthesia with ETI was also associated with poorer results in the K-ASQ.
Conclusion
Administration of general anesthesia with ETI to children is associated with an increased risk of ADHD and poor results in a neurodevelopmental screening test.
Figure
-
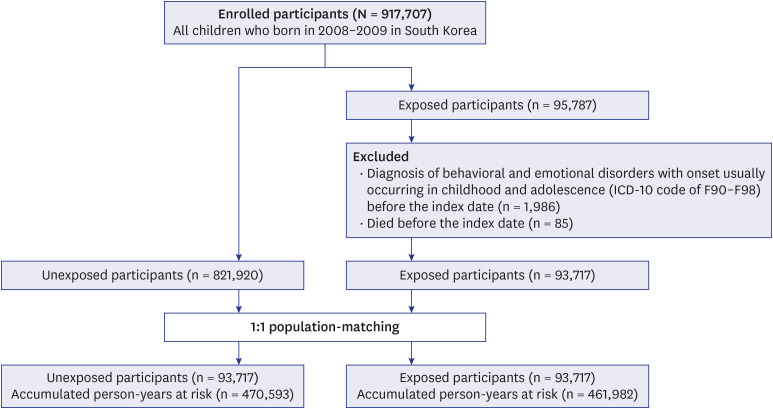
Fig. 1 Study design.ICD-10 = 10th revision of the International Classification of Diseases.
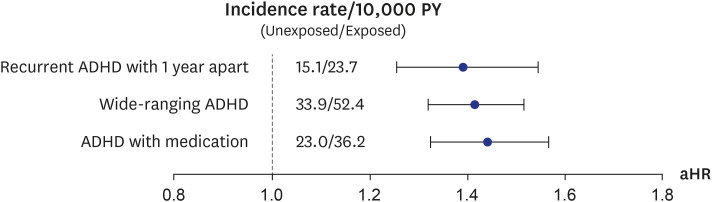
Fig. 2 Forest plot for sensitivity analysis of alternative definitions of ADHD. HRs and 95% CIs were calculated using a Cox proportional hazards model to assess the relationship between general anesthesia and various definitions of ADHD, adjusting for age at the index date, sex, calendar year of birth (2008 or 2009), birth weight, birth residence (Seoul/metropolitan, city, or rural area), economic status (low, middle, or high), and perinatal diseases. Recurrent ADHD 1 year apart was defined as two principal diagnoses of ICD-10 code F90.X after 72 months of age and 1 year apart between diagnoses. Wide-ranging ADHD was defined as at least a principal or second diagnosis of ICD-10 code F90.X after 72 months of age. ADHD with medication was defined as at least a principal diagnosis of ICD-10 code F90.X after 72 months of age with a prescription of methylphenidate. All outcomes were identified for at least one year (window period) after the index date. Filled rounds indicate aHRs and black lines indicate 95% CIs.ADHD = attention deficit hyperactivity disorder, PY = person-years, CI = confidence interval, HR = hazard ratio, aHR = adjusted hazard ratio, ICD-10 = 10th revision of the International Classification of Diseases.
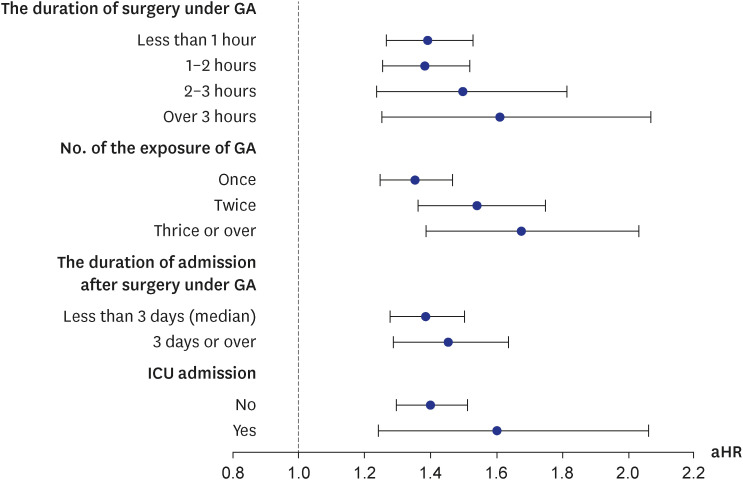
Fig. 3 Forest plot of the association between GA and ADHD according to the intensity of GA and participant’s condition after GA. HRs and 95% CIs were calculated using a Cox proportional hazards model, adjusting for age at the index date, sex, calendar year of birth (2008 or 2009), birth weight, birth residence (Seoul, metropolitan, city, or rural area), economic status (low, middle, or high), and perinatal diseases. To estimate the intensity of GA and participants’ condition after GA, the exposure was divided according to the duration of GA (less than 1 hour, 1–2 hours, 2–3 hours, or over 3 hours), number of GA exposures (once, twice, or thrice or over), duration of admission at the time of GA (less than 3 days [median] or 3 days or over), and admission to the ICU (yes or no). All outcomes were identified for at least one year (window period) after the index date. Filled rounds indicate aHRs and black lines indicate 95% CIs.ADHD = attention deficit hyperactivity disorder, CI = confidence interval, aHR = adjusted hazard ratio, ICU = intensive care unit, GA = general anesthesia.
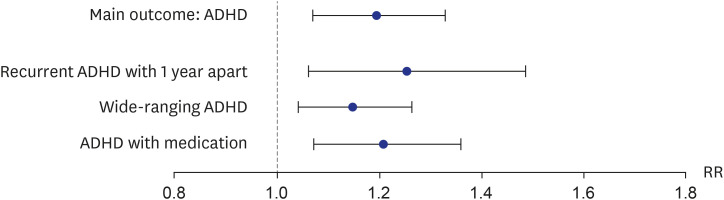
Fig. 4 Sensitivity analysis for the association between general anesthesia and ADHD based on the 1:1 propensity score matching method. RRs and 95% CIs were calculated using a modified Poisson regression to assess the relationship between general anesthesia and ADHD in the second cohort. ADHD as main outcome was defined as at least a principal diagnosis of ICD-10 code F90.X after 72 months old. Recurrent ADHD 1 year apart was defined as two principal diagnoses of ICD-10 code F90.X after 72 months of age and 1 year apart between diagnoses. Wide-ranging ADHD was defined as at least a principal or second diagnosis of ICD-10 code F90.X after 72 months of age. ADHD with medication was defined as at least a principal diagnosis of ICD-10 code F90.X after 72 months of age with a prescription of methylphenidate. All outcomes were identified for at least one year (window period) after the index date. Filled rounds indicate aRRs and black lines indicate 95% CIs.ADHD = attention deficit hyperactivity disorder, CI = confidence interval, RR = risk ratio, aRR = adjusted risk ratio, ICD-10 = 10th revision of the International Classification of Diseases.
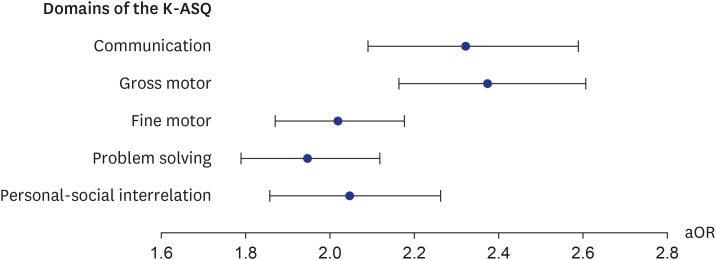
Fig. 5 Forest plot for the association between general anesthesia and each domain of K-ASQ. ORs and their 95% CIs were calculated using generalized estimated equations with the logit link function to assess the associations between general anesthesia exposure and adverse results of the K-ASQ in children. The results of each domain were stratified into appropriate, need for follow-up, and recommendations for further evaluation categories. The results of need for follow-up and recommendation for further evaluation, which mean a score below −1 and −2 standard deviations for age, were considered adverse results. All outcomes were identified for at least one year (window period) after the index date. Filled rounds indicate aORs and black lines indicate 95% CIs.K-ASQ = Korean-Ages and Stages Questionnaire, CI = confidence interval, OR = odds ratio, aOR = adjusted odds ratio.
Reference
-
1. U.S. Food and Drug Administration. FDA Drug Safety Communication: FDA Review Results in New Warnings About Using General Anesthetics and Sedation Drugs in Young Children and Pregnant Women. Silver Spring, MD, USA: U.S. Food and Drug Administration;2017.2. Shi Y, Hu D, Rodgers EL, Katusic SK, Gleich SJ, Hanson AC, et al. Epidemiology of general anesthesia prior to age 3 in a population-based birth cohort. Paediatr Anaesth. 2018; 28(6):513–519. PMID: 29532559.
Article3. Walkden GJ, Gill H, Davies NM, Peters AE, Wright I, Pickering AE. Early childhood general anesthesia and neurodevelopmental outcomes in the Avon Longitudinal Study of parents and children birth cohort. Anesthesiology. 2020; 133(5):1007–1020. PMID: 32898216.
Article4. Korean Statistical Information Service. KOSIS statistical database. Updated 2022. Accessed August 10th, 2022. https://kosis.kr/eng/ .5. Sanders RD, Hassell J, Davidson AJ, Robertson NJ, Ma D. Impact of anaesthetics and surgery on neurodevelopment: an update. Br J Anaesth. 2013; 110(Suppl 1):Suppl 1. i53–i72. PMID: 23542078.
Article6. Walters JL, Paule MG. Review of preclinical studies on pediatric general anesthesia-induced developmental neurotoxicity. Neurotoxicol Teratol. 2017; 60:2–23. PMID: 27871903.
Article7. Andersen SL. Trajectories of brain development: point of vulnerability or window of opportunity? Neurosci Biobehav Rev. 2003; 27(1-2):3–18. PMID: 12732219.
Article8. Lin EP, Lee JR, Lee CS, Deng M, Loepke AW. Do anesthetics harm the developing human brain? An integrative analysis of animal and human studies. Neurotoxicol Teratol. 2017; 60:117–128. PMID: 27793659.
Article9. McCann ME, de Graaff JC, Dorris L, Disma N, Withington D, Bell G, et al. Neurodevelopmental outcome at 5 years of age after general anaesthesia or awake-regional anaesthesia in infancy (GAS): an international, multicentre, randomised, controlled equivalence trial. Lancet. 2019; 393(10172):664–677. PMID: 30782342.10. Warner DO, Zaccariello MJ, Katusic SK, Schroeder DR, Hanson AC, Schulte PJ, et al. Neuropsychological and behavioral outcomes after exposure of young children to procedures requiring general anesthesia: the Mayo Anesthesia Safety in Kids (MASK) study. Anesthesiology. 2018; 129(1):89–105. PMID: 29672337.
Article11. Hu D, Flick RP, Zaccariello MJ, Colligan RC, Katusic SK, Schroeder DR, et al. Association between exposure of young children to procedures requiring general anesthesia and learning and behavioral outcomes in a population-based birth cohort. Anesthesiology. 2017; 127(2):227–240. PMID: 28609302.
Article12. Kim JH, Lee JE, Shim SM, Ha EK, Yon DK, Kim OH, et al. Cohort profile: national investigation of birth cohort in Korea study 2008 (NICKs-2008). Clin Exp Pediatr. 2021; 64(9):480–488. PMID: 33445832.
Article13. Gruschow SM, Yerys BE, Power TJ, Durbin DR, Curry AE. Validation of the use of electronic health records for classification of ADHD status. J Atten Disord. 2016; 23(13):1647–1655. PMID: 28112025.
Article14. Shi Y, Dykhoff HJ, Guevara LR, Sangaralingham LR, Schroeder DR, Flick RP, et al. Moderators of the association between attention-deficit/hyperactivity disorder and exposure to anaesthesia and surgery in children. Br J Anaesth. 2021; 127(5):722–728. PMID: 34503832.
Article15. Tsai CJ, Lee CT, Liang SH, Tsai PJ, Chen VC, Gossop M. Risk of ADHD after multiple exposures to general anesthesia: a nationwide retrospective cohort study. J Atten Disord. 2018; 22(3):229–239. PMID: 26023173.
Article16. Ko WR, Liaw YP, Huang JY, Zhao DH, Chang HC, Ko PC, et al. Exposure to general anesthesia in early life and the risk of attention deficit/hyperactivity disorder development: a nationwide, retrospective matched-cohort study. Paediatr Anaesth. 2014; 24(7):741–748. PMID: 24612161.
Article17. Grabowski J, Goldin A, Arthur LG, Beres AL, Guner YS, Hu YY, et al. The effects of early anesthesia on neurodevelopment: a systematic review. J Pediatr Surg. 2021; 56(5):851–861. PMID: 33509654.
Article18. Davidson AJ, Disma N, de Graaff JC, Withington DE, Dorris L, Bell G, et al. Neurodevelopmental outcome at 2 years of age after general anaesthesia and awake-regional anaesthesia in infancy (GAS): an international multicentre, randomised controlled trial. Lancet. 2016; 387(10015):239–250. PMID: 26507180.
Article19. McCann ME, Soriano SG. Does general anesthesia affect neurodevelopment in infants and children? BMJ. 2019; 367:l6459. PMID: 31818811.
Article20. Briner A, De Roo M, Dayer A, Muller D, Habre W, Vutskits L. Volatile anesthetics rapidly increase dendritic spine density in the rat medial prefrontal cortex during synaptogenesis. Anesthesiology. 2010; 112(3):546–556. PMID: 20124985.
Article21. Vutskits L. General anesthesia: a gateway to modulate synapse formation and neural plasticity? Anesth Analg. 2012; 115(5):1174–1182. PMID: 22859689.22. Zhang LL, Pathak HR, Coulter DA, Freed MA, Vardi N. Shift of intracellular chloride concentration in ganglion and amacrine cells of developing mouse retina. J Neurophysiol. 2006; 95(4):2404–2416. PMID: 16371454.
Article23. Edwards DA, Shah HP, Cao W, Gravenstein N, Seubert CN, Martynyuk AE. Bumetanide alleviates epileptogenic and neurotoxic effects of sevoflurane in neonatal rat brain. Anesthesiology. 2010; 112(3):567–575. PMID: 20124973.
Article24. Dalla Massara L, Osuru HP, Oklopcic A, Milanovic D, Joksimovic SM, Caputo V, et al. General anesthesia causes epigenetic histone modulation of c-Fos and brain-derived neurotrophic factor, target genes important for neuronal development in the immature rat hippocampus. Anesthesiology. 2016; 124(6):1311–1327. PMID: 27028464.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Report of a Child who has Attention Deficit Hyperactivity Disorder, Mental Retardation, and Mania
- Association between the Brain-Derived Neurotropic Factor and Attention Deficit Hyperactivity Disorder
- OROS Methylphenidate Treatment of Secondary Adult ADHD after Traumatic Brain Injury
- Childhood Attention Deficit in the Patients with Bipolar Disorder and CHRNA7 Gene Polymorphisms
- Factors related to Medication Adherence according to Severity of Attention Deficit Hyperactivity Disorder in Children
