Secondary hyperparathyroidism due to multiple parathyroid carcinomas in a patient with chronic hemodialysis: a case report
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Pusan National University Hospital, Busan, Korea
- 2Division of Nephrology, Department of Internal Medicine, Pusan National University Hospital, Busan, Korea
- 3Department of Otorhinolaryngology-Head and Neck Surgery, Pusan National University Hospital, Busan, Korea
- KMID: 2538806
- DOI: http://doi.org/10.7180/kmj.22.103
Abstract
- Parathyroid carcinoma (PC) in cases of secondary or tertiary hyperparathyroidism is relatively uncommon, and only a few case reports have described this entity. Although some papers have reported patients with one or two parathyroid malignancies, multiple PC–especially three or more–have been even more rarely reported. Herein, we report a case of secondary hyperparathyroidism due to multiple PCs in a chronic hemodialysis patient. A 54-year-old man with end-stage kidney disease was referred for hyperparathyroidism. He had been diagnosed with chronic kidney disease in 2001 and had begun hemodialysis in 2009. In laboratory tests, intact parathyroid hormone (iPTH) was markedly elevated to 1,144.1 pg/mL (normal range: 15.0–68.3 pg/mL) and serum calcium was mildly elevated to 10.56 mg/dL (normal range: 8.5–10.3 mg/dL). Ultrasonography showed hypoechoic nodules in the posterior part of both thyroid glands. All three nodules showed increased uptake on a 99mTc sestamibi scan. The patient underwent total parathyroidectomy with autotransplantation to the right forearm. Histopathology findings showed three PCs with capsular invasion and one parathyroid hyperplasia. In the immediate postoperative period, the iPTH level dropped from 1,446.8 to 82.4 pg/dL and, after 1 month, to 4.0 pg/dL. This patient needed oral calcium carbonate and active vitamin D to maintain appropriate serum calcium levels. Although multiple PCs are rare, they can cause secondary hyperparathyroidism. Therefore, clinicians should suspect multiple PCs when patients’ serum iPTH levels are exceptionally high. Additionally, since PCs could occur in multiple glands, autotransplantation of the parathyroid gland after parathyroidectomy should be done carefully.
Keyword
Figure
-
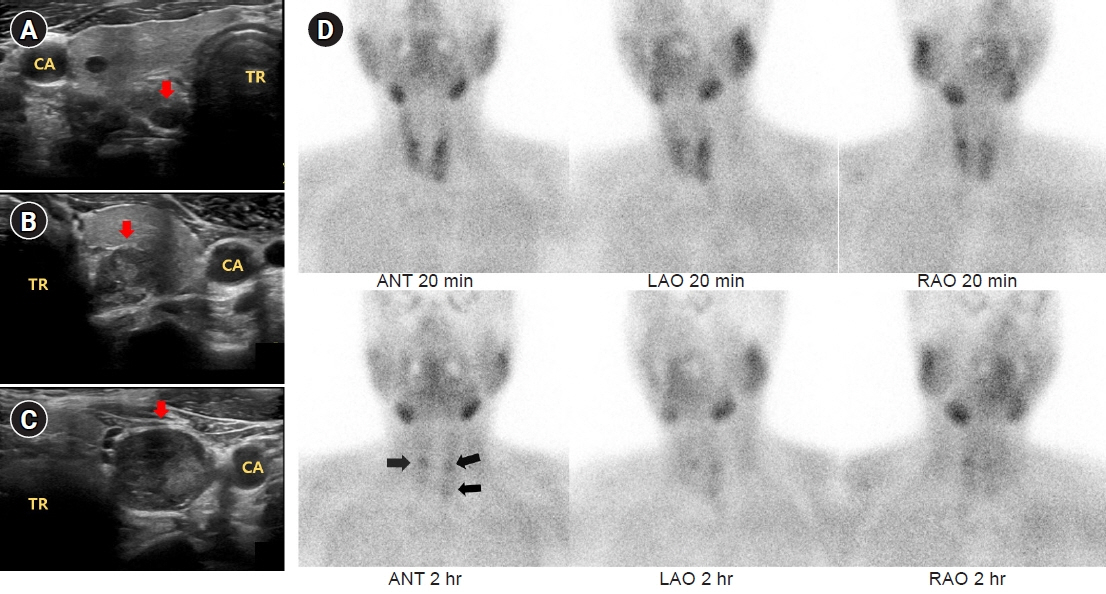
Fig. 1. Ultrasonography and 99mTc sestamibi single photon emission computed tomography (SPECT) of parathyroid glands (arrow). (A) Right superior parathyroid gland. (B) Left superior parathyroid gland. (C) Left inferior parathyroid gland. (D) Parathyroid SPECT images acquired 20 minutes and 2 hours after the intravenous 99mTc sestamibi injection. CA, carotid artery; TR, trachea, ANT, anterior; LAO, left anterior oblique; RAO, right anterior oblique.
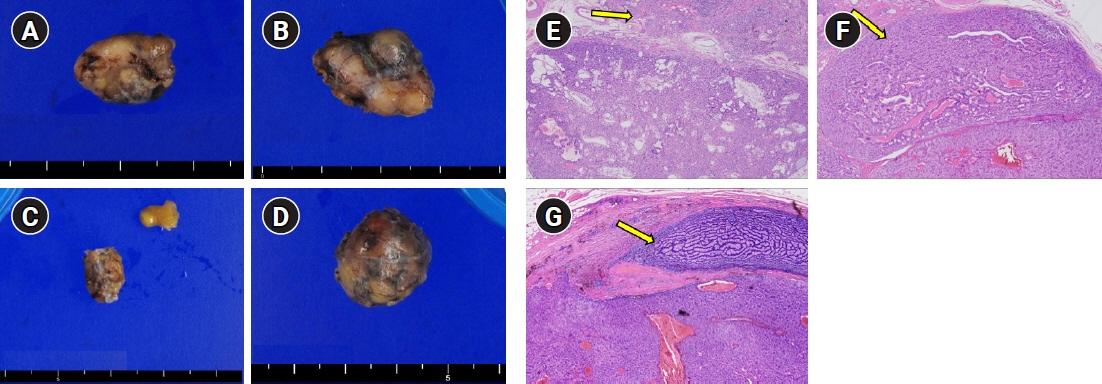
Fig. 2. Postoperative gross and microscopic histology of each parathyroid gland. Gross pathology images of (A) the right superior parathyroid gland, (B) the left superior parathyroid gland, (C) the right inferior parathyroid gland, and (D) the left inferior parathyroid gland. Microscopic examinations of three parathyroid carcinomas: (E) right superior parathyroid gland (H&E, ×40), (F) left superior parathyroid gland (H&E, ×40), (G) left inferior parathyroid gland (H&E, ×40). Capsular invasion is indicated by an arrow.
Reference
-
References
1. McClenaghan F, Qureshi YA. Parathyroid cancer. Gland Surg. 2015; 4:329–38.2. Shane E. Clinical review 122: parathyroid carcinoma. J Clin Endocrinol Metab. 2001; 86:485–93.3. Belafsky PC. Current opinion in otolaryngology & head & neck surgery: editorial comment. Curr Opin Otolaryngol Head Neck Surg. 2009; 17:419.4. Habas E Sr, Eledrisi M, Khan F, Elzouki AY. Secondary hyperparathyroidism in chronic kidney disease: pathophysiology and management. Cureus. 2021; 13:e16388.5. Machado NN, Wilhelm SM. Parathyroid cancer: a review. Cancers (Basel). 2019; 11:1676.6. Cao J, Chen C, Wang QL, Xu JJ, Ge MH. Parathyroid carcinoma: a report of six cases with a brief review of the literature. Oncol Lett. 2015; 10:3363–8.7. Kada S, Tanaka M, Yasoda A. Parathyroid carcinoma in a patient with secondary hyperparathyroidism and thyroid hemiagenesis: a case report and review of the literature. Ear Nose Throat J. 2021; Jul. 28. https://doi.org/10.1177/01455613211036240.8. Duan K, Mete O. Parathyroid carcinoma: diagnosis and clinical implications. Turk Patoloji Derg. 2015; 31 Suppl 1:80–97.9. Kowalski GJ, Bednarczyk A, Bula G, Gawrychowska A, Gawrychowski J. Parathyroid carcinoma: a study of 29 cases. Endokrynol Pol. 2022; 73:56–63.10. Wen P, Xu L, Zhao S, Gan W, Hou D, Zhang L, et al. Risk factors for severe hypocalcemia in patients with secondary hyperparathyroidism after total parathyroidectomy. Int J Endocrinol. 2021; 2021:6613659.11. Haciyanli M, Oruk G, Ucarsoy AA, Gur O, Genc H, Krikorian A, et al. Multiglandular parathyroid carcinoma: case report and review of the literature. Endocr Pract. 2011; 17:598–601.12. Oh SK, Park YH, Kim JH, Lee MS, Min HK. Multiple primary parathyroid carcinoma. J Korean Surg Soc. 1990; 39:546–53.13. Harari A, Waring A, Fernandez-Ranvier G, Hwang J, Suh I, Mitmaker E, et al. Parathyroid carcinoma: a 43-year outcome and survival analysis. J Clin Endocrinol Metab. 2011; 96:3679–86.14. Wei CH, Harari A. Parathyroid carcinoma: update and guidelines for management. Curr Treat Options Oncol. 2012; 13:11–23.15. Kebebew E. Parathyroid carcinoma. Curr Treat Options Oncol. 2001; 2:347–54.16. Lee PK, Jarosek SL, Virnig BA, Evasovich M, Tuttle TM. Trends in the incidence and treatment of parathyroid cancer in the United States. Cancer. 2007; 109:1736–41.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Surgical Experience of Secondary Hyperparathyroidism
- A Case of Newly Detected Ectopic Mediastinal Parathyroid Gland in Chronic Renal Failure Patient after Parathyroidectomy
- A Case of Brown Tumor of the Mandible Caused by Hyperparathyroidism
- A Case of Parathyroid Carcinoma Presenting as Brown Tumors
- Fibrous Dysplasia of the Jaws Associated with Secondary Hyperparathyroidism: A Case Report
