Trends and an Online Survey on the Use of Rigid Bronchoscopy in Korea
- Jeong BH
 1
1 - Lee SH2
- Kim HH2
- Yoon HI3
- Eom JS4
- Park YS5
- Cho J5
- Lee T6
- Kim SJ7
- Cho HJ7
- Park CK8
- Ko Y9
- Kwon YS10
- Kim C11
- Ji W12
- Choi CM12
- Seo KH13
- Nam HS14
- Kim H1
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 2Division of Pulmonary, Critical Care and Sleep Medicine, Department of Internal Medicine, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 3Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
- 4Department of Internal Medicine, Pusan National University School of Medicine, Busan, Korea
- 5Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
- 6Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea
- 7Division of Pulmonology, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 8Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 9Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
- 10Department of Internal Medicine, Chonnam National University Medical School, Chonnam National University Hospital, Gwangju, Korea
- 11Department of Internal Medicine, Jeju National University Hospital, Jeju National University School of Medicine, Jeju, Korea
- 12Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 13Division of Pulmonary and Critical Care Medicine, Department of Medicine, Soonchunhyang University Cheonan Hospital, Cheonan, Korea
- 14Division of Pulmonology, Department of Internal Medicine, Inha University Hospital, Inha University School of Medicine, Incheon, Korea
- KMID: 2538370
- DOI: http://doi.org/10.3346/jkms.2023.38.e13
Abstract
- Background
Although almost all interventional pulmonologists agree that rigid bronchoscopy is irreplaceable in the field of interventional pulmonology, less is known about the types of diseases that the procedure is used for and what difficulties the operators face during the procedure. The purpose of this study is to evaluate what diseases rigid bronchoscopy is used for, whether it is widely used, and what challenges the operators face in Korea.
Methods
We enrolled 14 hospitals in this retrospective cohort of patients who underwent rigid bronchoscopy between 2003 and 2020. An online survey was conducted with 14 operators to investigate the difficulties associated with the procedure.
Results
While the number of new patients at Samsung Medical Center (SMC) increased from 189 in 2003–2005 to 468 in 2018–2020, that of other institutions increased from 0 to 238. The proportion of SMC patients in the total started at 100% and steadily decreased to 59.2%. The proportion of malignancy as the indication for the procedure steadily increased from 29.1% to 43.0%, whereas post-tuberculous stenosis (25.4% to 12.9%) and post-intubation stenosis (19.0% to 10.9%) steadily decreased (all P for trends < 0.001). In the online survey, half of the respondents stated that over the past year they performed less than one procedure per month. The fewer the procedures performed within the last year, the more likely collaboration with other departments was viewed as a recent obstacle (Spearman correlation coefficient, r s = −0.740, P = 0.003) and recent administrative difficulties were encountered (r s = −0.616, P = 0.019).
Conclusion
This study demonstrated that the number of patients undergoing rigid bronchoscopy has been increasing, especially among cancer patients. For this procedure to be used more widely, it will be important for beginners to systematically learn about the procedure itself as well as to achieve multidisciplinary consultation.
Figure
-
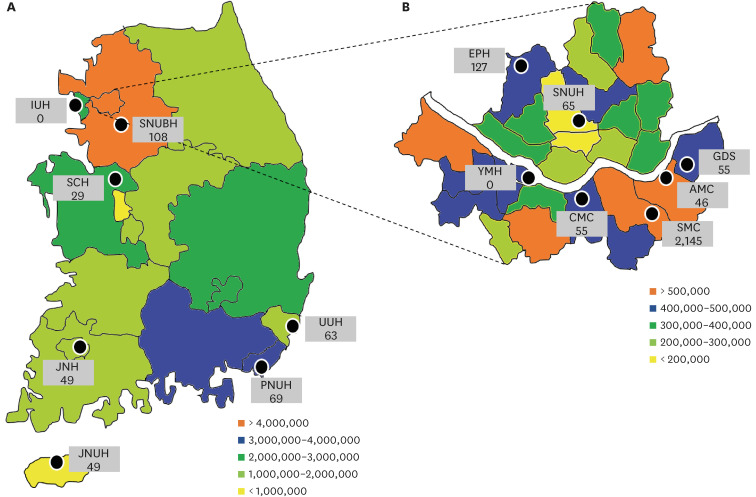
Fig. 1 Location of each hospital participating in this study. The number of populations in each region is indicated by color, and the number of patients included during the study period in each hospital is indicated by a number. Two hospitals (IUH and YMH) were unable to perform rigid bronchoscopy due to administrative problems and non-cooperation with other departments during the study period. The full name of each hospital is in the footnote of Supplementary Table 1. (A) The 17 administrative districts of the Republic of Korea. (B) The 25 administrative districts of Seoul are presented separately.
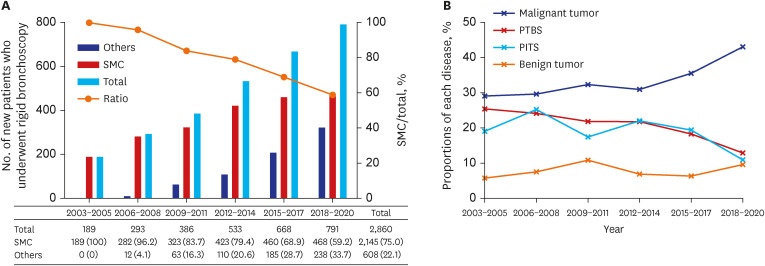
Fig. 2 Trends in the number of new patients and the indications for rigid bronchoscopy. (A) The trend in the number of new patients undergoing rigid bronchoscopy over time. Black and gray bars represent the numbers of new patients treated at SMC and hospitals other than SMC, respectively. Checkered bars indicate the total number of new patients who underwent the rigid bronchoscopy. A line graph shows the ratio of the number of patients at SMC to the total number of patients. See Supplementary Table 1 for detailed figures. (B) The trend in the indications for the rigid bronchoscopy. Red, purple, green, and gray lines represent malignant diseases, PTBS, PITS, and benign tumors, respectively. See Supplementary Table 2 for detailed figures.SMC = Samsung Medical Center, PTBS = post-tuberculosis tracheobronchial stenosis, PITS = post-intubation or tracheostomy tracheal stenosis.
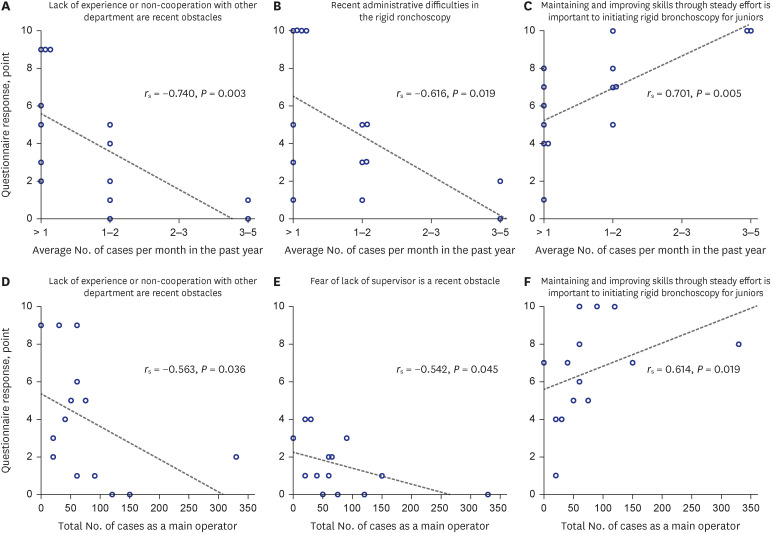
Fig. 3 Correlation between respondent characteristics and survey responses. The degree of correlation was expressed as a Spearman correlation coefficient value (r s). Generally, 0.40–0.59 is interpreted as ‘moderate’, 0.60–0.79 as ‘strong’, and 0.80–1.0 as ‘very strong’ relationships. Refer to Table 3 and Supplementary Data 1 for detailed survey content and the meaning of the survey responses of 0 to 10 points.
Reference
-
1. Batra H, Yarmus L. Indications and complications of rigid bronchoscopy. Expert Rev Respir Med. 2018; 12(6):509–520. PMID: 29727208.2. Dutau H, Vandemoortele T, Breen DP. Rigid bronchoscopy. Clin Chest Med. 2013; 34(3):427–435. PMID: 23993814.3. Dumon JF. A dedicated tracheobronchial stent. Chest. 1990; 97(2):328–332. PMID: 1688757.4. Dumon JF, Reboud E, Garbe L, Aucomte F, Meric B. Treatment of tracheobronchial lesions by laser photoresection. Chest. 1982; 81(3):278–284. PMID: 7056101.5. Kim HJ. Airway silicone stenting in the management of tracheobronchial stenosis. Tuberc Respir Dis (Seoul). 2007; 62(2):95–97.6. Bartlett-Pestell S, May J, Sharma A, Alonzo S, Barnes N, Madden BP. A 12-year experience in endobronchial intervention using rigid bronchoscopy - account of a tertiary referral centre. Monaldi Arch Chest Dis. 2022; 92(4):7. Kim HJ, Kim SW, Lee HY, Kang HH, Kang JY, Kim JS, et al. Clinical experience of rigid bronchoscopy in single center. Tuberc Respir Dis (Seoul). 2012; 72(6):486–492. PMID: 23101015.8. Mahmood K, Wahidi MM, Shepherd RW, Argento AC, Yarmus LB, Lee H, et al. Variable learning curve of basic rigid bronchoscopy in trainees. Respiration. 2021; 100(6):530–537. PMID: 33849039.9. Pathak V, Welsby I, Mahmood K, Wahidi M, MacIntyre N, Shofer S. Ventilation and anesthetic approaches for rigid bronchoscopy. Ann Am Thorac Soc. 2014; 11(4):628–634. PMID: 24635585.10. Korea Disease Control and Prevention Agency. Annual report on the notified tuberculosis in Korea, 2021. Updated 2021. Accessed August 14, 2022. https://www.kdca.go.kr/index.es?sid=a3 .11. Ministry of Health and Welfare, Korea Central Cancer Registry, National Cancer Center. Annual report of cancer statistics in Korea in 2016. Updated 2018. Accessed August 14, 2022. https://ncc.re.kr/main.ncc?uri=english/sub04_Statistics .12. Myer CM 3rd, O’Connor DM, Cotton RT. Proposed grading system for subglottic stenosis based on endotracheal tube sizes. Ann Otol Rhinol Laryngol. 1994; 103(4 Pt 1):319–323. PMID: 8154776.13. Prakash UB, Offord KP, Stubbs SE. Bronchoscopy in North America: the ACCP survey. Chest. 1991; 100(6):1668–1675. PMID: 1959412.14. Colt HG, Prakash UBS, Offord KP. Bronchoscopy in North America: survey by the American Association for Bronchology, 1999. J Bronchology Interv Pulmonol. 2000; 7(1):8–25.15. Shin B, Chang B, Kim H, Jeong BH. Interventional bronchoscopy in malignant central airway obstruction by extra-pulmonary malignancy. BMC Pulm Med. 2018; 18(1):46. PMID: 29534706.16. Kim BG, Lee K, Um SW, Han J, Cho JH, Kim J, et al. Clinical outcomes and the role of bronchoscopic intervention in patients with primary pulmonary salivary gland-type tumors. Lung Cancer. 2020; 146:58–65. PMID: 32512274.17. Kim BG, Shin B, Chang B, Kim H, Jeong BH. Prognostic factors for survival after bronchoscopic intervention in patients with airway obstruction due to primary pulmonary malignancy. BMC Pulm Med. 2020; 20(1):54. PMID: 32103738.18. Ryu YJ, Kim H, Yu CM, Choi JC, Kwon YS, Kwon OJ. Use of silicone stents for the management of post-tuberculosis tracheobronchial stenosis. Eur Respir J. 2006; 28(5):1029–1035. PMID: 16971412.19. Lim SY, Park HK, Jeon K, Um SW, Koh WJ, Suh GY, et al. Factors predicting outcome following airway stenting for post-tuberculosis tracheobronchial stenosis. Respirology. 2011; 16(6):959–964. PMID: 21605277.20. Eom JS, Kim H, Park HY, Jeon K, Um SW, Koh WJ, et al. Timing of silicone stent removal in patients with post-tuberculosis bronchial stenosis. Ann Thorac Med. 2013; 8(4):218–223. PMID: 24250736.21. Rosell A, Stratakos G. Therapeutic bronchoscopy for central airway diseases. Eur Respir Rev. 2020; 29(158):190178. PMID: 33208484.22. Johnson RF, Bradshaw S, Jaffal H, Chorney SR. Estimations of laryngotracheal stenosis after mechanical ventilation: a cross-sectional analysis. Laryngoscope. 2022; 132(9):1723–1728. PMID: 34542167.23. Dorris ER, Russell J, Murphy M. Post-intubation subglottic stenosis: aetiology at the cellular and molecular level. Eur Respir Rev. 2021; 30(159):200218. PMID: 33472959.24. Ost DE, Ernst A, Grosu HB, Lei X, Diaz-Mendoza J, Slade M, et al. Complications following therapeutic bronchoscopy for malignant central airway obstruction: results of the AQuIRE Registry. Chest. 2015; 148(2):450–471. PMID: 25741903.25. Ost DE, Ernst A, Grosu HB, Lei X, Diaz-Mendoza J, Slade M, et al. Therapeutic bronchoscopy for malignant central airway obstruction: success rates and impact on dyspnea and quality of life. Chest. 2015; 147(5):1282–1298. PMID: 25358019.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dexmedetomidine for Rigid Bronchoscopy in an Infant with Tracheal Web after Ventricular Septal Defect Patch Repair
- Airway fire injury during rigid bronchoscopy in a patient with a silicon stent: A case report
- A Case of Tracheal Carcinoma Diagnosed by Rigid Bronchoscopy in Lidocaine Anaphylaxis Patient
- An endobronchial hamartoma removed via rigid bronchoscopy under general anesthesia
- Rigid Bronchoscopy for Post-Tuberculosis Tracheobronchial Stenosis
