J Korean Neurosurg Soc.
2023 Jan;66(1):95-104. 10.3340/jkns.2022.0161.
Clinical Outcomes Associated with Degree of Hypernatremia in Neurocritically Ill Patients
- Affiliations
-
- 1Department of Internal Medicine, National Cancer Center, Goyang, Korea
- 2Statistic and Data Center, Clinical Research Institute, Samsung Medical Center, Seoul, Korea
- 3Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 4Department of Neurosurgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2537853
- DOI: http://doi.org/10.3340/jkns.2022.0161
Abstract
Objective
: Hypernatremia is a common complication encountered during the treatment of neurocritically ill patients. However, it is unclear whether clinical outcomes correlate with the severity of hypernatremia in such patients. Therefore, we investigated the impact of hypernatremia on mortality of these patients, depending on the degree of hypernatremia.
Methods
: Among neurosurgical patients admitted to the intensive care unit (ICU) in a tertiary hospital from January 2013 to December 2019, patients who were hospitalized in the ICU for more than 5 days and whose serum sodium levels were obtained during ICU admission were included. Hypernatremia was defined as the highest serum sodium level exceeding 150 mEq/L observed. We classified the patients into four subgroups according to the severity of hypernatremia and performed propensity score matching analysis.
Results
: Among 1146 patients, 353 patients (30.8%) showed hypernatremia. Based on propensity score matching, 290 pairs were included in the analysis. The hypernatremia group had higher rates of in-hospital mortality and 28-day mortality in both overall and matched population (both p<0.001 and p=0.001, respectively). In multivariable analysis of propensity score-matched population, moderate and severe hypernatremia were significantly associated with in-hospital mortality (adjusted odds ratio [OR], 4.58; 95% confidence interval [CI], 2.15–9.75 and adjusted OR, 6.93; 95% CI, 3.46–13.90, respectively) and 28-day mortality (adjusted OR, 3.51; 95% CI, 1.54–7.98 and adjusted OR, 10.60; 95% CI, 5.10–21.90, respectively) compared with the absence of hypernatremia. However, clinical outcomes, including in-hospital mortality and 28-day mortality, were not significantly different between the group without hypernatremia and the group with mild hypernatremia (p=0.720 and p=0.690, respectively). The mortality rates of patients with moderate and severe hypernatremia were significantly higher in both overall and matched population. Interestingly, the mild hypernatremia group of matched population showed the best survival rate.
Conclusion
: Moderate and severe hypernatremia were associated with poor clinical outcomes in neurocritically ill patients. However, the prognosis of patients with mild hypernatremia was similar with that of patients without hypernatremia. Therefore, mild hypernatremia may be allowed during treatment of intracranial hypertension using hyperosmolar therapy.
Keyword
Figure
-
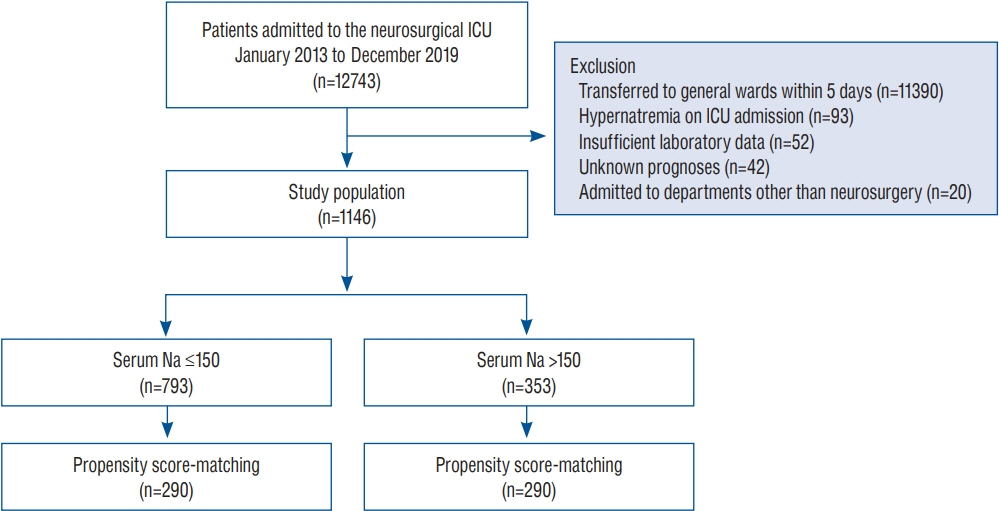
Fig. 1. Study flow chart. ICU : intensive care unit, Na : sodium level.
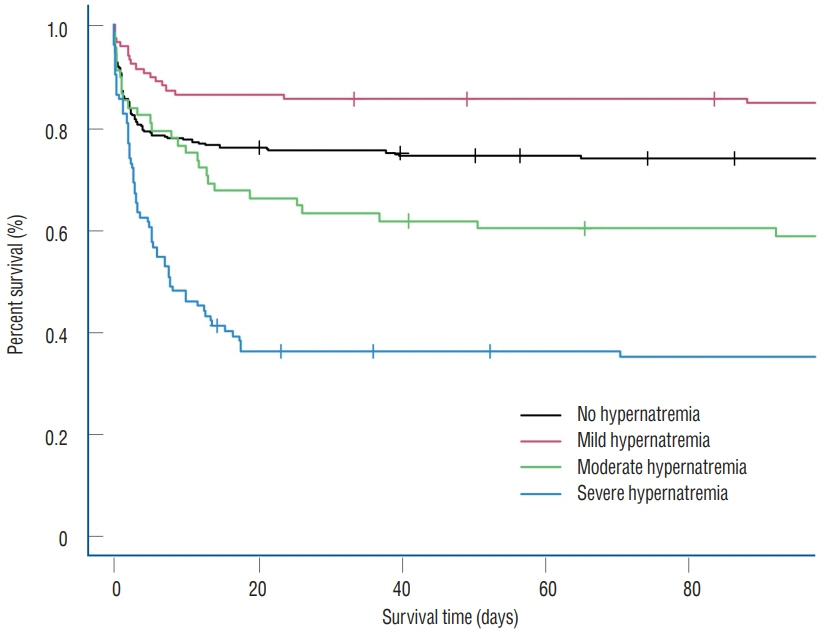
Fig. 2. Kaplan-Meier survival analyses of propensity score-mached population (p<0.001).
Reference
-
References
1. Aiyagari V, Deibert E, Diringer MN. Hypernatremia in the neurologic intensive care unit: how high is too high? J Crit Care. 21:163–172. 2006.2. Andrews PM, Cooper M, Verbesey J, Ghasemian S, Rogalsky D, Moody P, et al. Mannitol infusion within 15 min of cross-clamp improves living donor kidney preservation. Transplantation. 98:893–897. 2014.3. Austin PC. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 10:150–161. 2011.4. Ayus JC, Armstrong DL, Arieff AI. Effects of hypernatraemia in the central nervous system and its therapy in rats and rabbits. J Physiol. 492 (Pt 1):243–255. 1996.5. Beseoglu K, Etminan N, Steiger HJ, Hänggi D. The relation of early hypernatremia with clinical outcome in patients suffering from aneurysmal subarachnoid hemorrhage. Clin Neurol Neurosurg. 123:164–168. 2014.6. Capuzzo M, Valpondi V, Sgarbi A, Bortolazzi S, Pavoni V, Gilli G, et al. Validation of severity scoring systems SAPS II and APACHE II in a singlecenter population. Intensive Care Med. 26:1779–1785. 2000.7. Choi HW, Yoon CH, Ryu JA. Acute kidney injury following mannitol infusion in neurosurgical patients. J Neurointensive Care. 5:9–14. 2022.8. Darmon M, Timsit JF, Francais A, Nguile-Makao M, Adrie C, Cohen Y, et al. Association between hypernatraemia acquired in the ICU and mortality: a cohort study. Nephrol Dial Transplant. 25:2510–2515. 2010.9. Fink ME. Osmotherapy for intracranial hypertension: mannitol versus hypertonic saline. Continuum (Minneap Minn). 18:640–654. 2012.10. Hu B, Han Q, Mengke N, He K, Zhang Y, Nie Z, et al. Prognostic value of ICU-acquired hypernatremia in patients with neurological dysfunction. Medicine (Baltimore). 95:e3840. 2016.11. Imaizumi T, Nakatochi M, Fujita Y, Nomura R, Watanabe K, Maekawa M, et al. The association between intensive care unit-acquired hypernatraemia and mortality in critically ill patients with cerebrovascular diseases: a single-centre cohort study in Japan. BMJ Open. 7:e016248. 2017.12. Jeon SB, Koh Y, Choi HA, Lee K. Critical care for patients with massive ischemic stroke. J Stroke. 16:146–160. 2014.13. Kim MY, Park JH, Kang NR, Jang HR, Lee JE, Huh W, et al. Increased risk of acute kidney injury associated with higher infusion rate of mannitol in patients with intracranial hemorrhage. J Neurosurg. 120:1340–1348. 2014.14. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 13:818–829. 1985.15. Kolmodin L, Sekhon MS, Henderson WR, Turgeon AF, Griesdale DE. Hypernatremia in patients with severe traumatic brain injury: a systematic review. Ann Intensive Care. 3:35. 2013.16. Li M, Hu YH, Chen G. Hypernatremia severity and the risk of death after traumatic brain injury. Injury. 44:1213–1218. 2013.17. Lindner G, Funk GC. Hypernatremia in critically ill patients. J Crit Care. 28:216.e11–20. 2013.18. Lindner G, Funk GC, Lassnigg A, Mouhieddine M, Ahmad SA, Schwarz C, et al. Intensive care-acquired hypernatremia after major cardiothoracic surgery is associated with increased mortality. Intensive Care Med. 36:1718–1723. 2010.19. Lindner G, Funk GC, Schwarz C, Kneidinger N, Kaider A, Schneeweiss B, et al. Hypernatremia in the critically ill is an independent risk factor for mortality. Am J Kidney Dis. 50:952–957. 2007.20. Maggiore U, Picetti E, Antonucci E, Parenti E, Regolisti G, Mergoni M, et al. The relation between the incidence of hypernatremia and mortality in patients with severe traumatic brain injury. Crit Care. 13:R110. 2009.21. Meredith W, Rutledge R, Fakhry SM, Emery S, Kromhout-Schiro S. The conundrum of the Glasgow coma scale in intubated patients: a linear regression prediction of the Glasgow verbal score from the Glasgow eye and motor scores. J Trauma. 44:839–844. discussion 844-845. 1998.22. O'Donoghue SD, Dulhunty JM, Bandeshe HK, Senthuran S, Gowardman JR. Acquired hypernatraemia is an independent predictor of mortality in critically ill patients. Anaesthesia. 64:514–520. 2009.23. Polderman KH, Schreuder WO, Strack van Schijndel RJ, Thijs LG. Hypernatremia in the intensive care unit: an indicator of quality of care? Crit Care Med. 27:1105–1108. 1999.24. Qureshi AI, Suarez JI, Bhardwaj A, Mirski M, Schnitzer MS, Hanley DF, et al. Use of hypertonic (3%) saline/acetate infusion in the treatment of cerebral edema: effect on intracranial pressure and lateral displacement of the brain. Crit Care Med. 26:440–446. 1998.25. Sim JK, Ko RE, Na SJ, Suh GY, Jeon K. Intensive care unit-acquired hyponatremia in critically ill medical patients. J Transl Med. 18:268. 2020.26. Vedantam A, Robertson CS, Gopinath SP. Morbidity and mortality associated with hypernatremia in patients with severe traumatic brain injury. Neurosurg Focus. 43:E2. 2017.27. Waite MD, Fuhrman SA, Badawi O, Zuckerman IH, Franey CS. Intensive care unit-acquired hypernatremia is an independent predictor of increased mortality and length of stay. J Crit Care. 28:405–412. 2013.28. Wells DL, Swanson JM, Wood GC, Magnotti LJ, Boucher BA, Croce MA, et al. The relationship between serum sodium and intracranial pressure when using hypertonic saline to target mild hypernatremia in patients with head trauma. Crit Care. 16:R193. 2012.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prognostic Value of Early Hyperglycemia in Neurocritically Ill Patients
- Impact of Critical Care Registered Dietitian on Clinical Outcomes of Neurocritically Ill Patients
- Principle of intravenous fluid therapy in the neurocritically ill patients
- Neostigmine for Treating Acute Colonic Pseudo-Obstruction in Neurocritically Ill Patients
- Association of Obesity With Clinical Outcomes in Neurocritically Ill Patients
