Clinical course in children with equivocal appendicitis on computed tomography: a retrospective cohort study
- Affiliations
-
- 1Department of Surgery, Seoul National University Bundang Hospital, Seongnam, Korea
- 2Department of Surgery, Ewha Womans University Seoul Hospital, Seoul, Korea
- 3Department of Pediatric Surgery, Seoul National University Children’s Hospital, Seoul, Korea
- 4Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea
- 5Department of Surgery, College of Medicine, Seoul National University, Seoul, Korea
- KMID: 2537630
- DOI: http://doi.org/10.4174/astr.2023.104.1.51
Abstract
- Purpose
Appendectomy is one of the most common surgeries in children. Although various radiological examinations are performed, they do not always reveal a definitive diagnosis of appendicitis. This study aimed to investigate the clinical course of equivocal appendicitis, identify the factors associated with appendectomy, and suggest appropriate management for these patients.
Methods
Patients younger than 19 years who visited Seoul National University Bundang Hospital with a differential diagnosis of appendicitis from January 2013 to December 2017 were included. All participants conducted ‘appendiceal CT’ with a scoring scale of 1–5. The higher the score, the higher the likelihood of a radiologic diagnosis of appendicitis. We defined the appendicitis CT score of 2–4 as equivocal appendicitis (n = 143). Medical records were reviewed retrospectively for demographics, further examination as abdominal ultrasonography, and appendectomy status (yes or no). The mean follow-up period was 15.6 ± 71 days.
Results
Equivocal appendicitis accounted for 16.7%. Additional ultrasonography test was performed in 24.5% (35 of 143). In total, 34 patients (23.8%) underwent appendectomy. Among the patients with appendiceal CT scores 2, 3, and 4, 4.9%, 50.0%, and 87.5% underwent appendectomy, respectively. Higher WBC count, higher appendicitis CT score, and readmission were significantly associated with appendectomy in patients with equivocal appendicitis.
Conclusion
Higher appendicitis CT score and WBC level were positively associated with appendectomy. Careful observation can be a treatment option in appendicitis CT score 2 or 3 groups. Appendectomy is the first-line treatment for patients with appendicitis score 4. Additional ultrasonography test is advisable to determine treatment modality for equivocal appendicitis.
Keyword
Figure
-
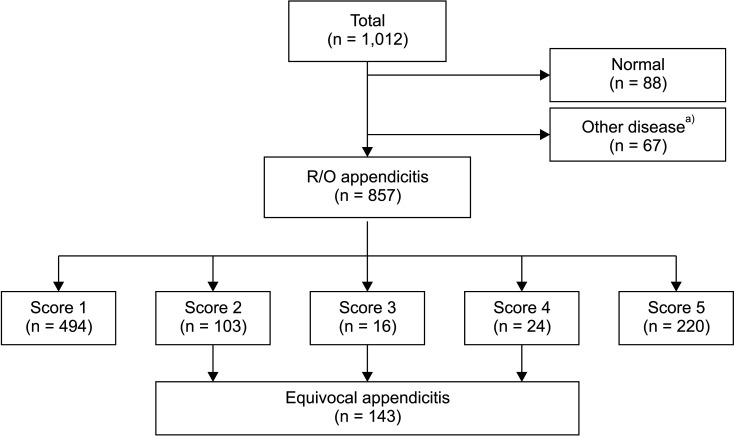
Fig. 1 Patient collection. Patients with appendicitis CT scores of 2 to 4 were enrolled in the study. R/O, rule out. a)Enterocolitis, 24; ovary cyst, 8; urinary abnormality, 6; ileus, 6; diverticulitis, 3; pancreatitis, 2; superior mesenteric artery syndrome, 2; upper gastrointestinal perforation, 2; intussusception, 2; omental infarction, 2; intestinal duplication, 1; hepatitis, 1; pancreatitis, 1; Meckel’s diverticulitis, 1; juvenile polyp, 1; foreign body, 1; solid pseudopapillary tumor, 1; uterine myoma, 1; psoas myositis, 1; empyema, 1.
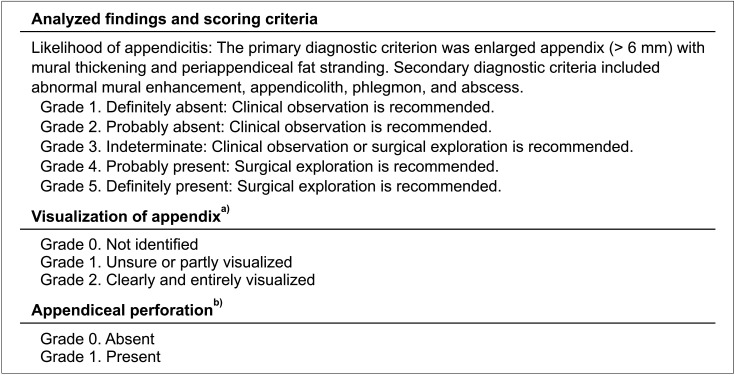
Fig. 2 Appendiceal CT report format. a)In cases with phlegmon or abscess, grade 2 was assigned if there was clear continuity between the lesion and the remaining appendiceal base, indicating that the lesion had originated from the appendix. b)Based on findings of extraluminal gas or appendicolith, periappendiceal fluid or phlegm on, severe periappendiceal fat stranding, and defect in the appendiceal wall.

Fig. 3 Examples of appendiceal CT images of equivocal appendicitis (arrows). (A) Score 2, (B) score 3, and (C) score 4.
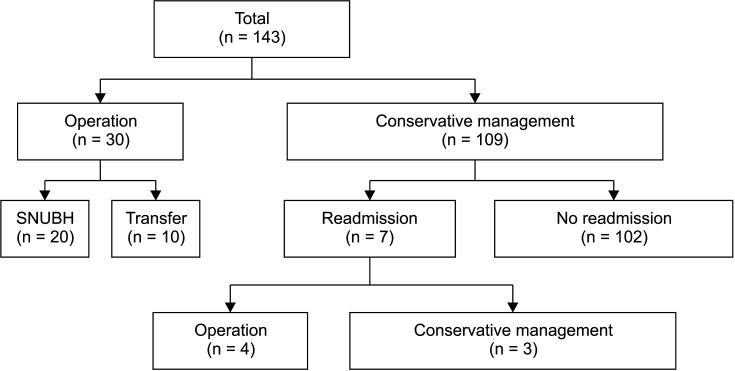
Fig. 4 Clinical course of patients with equivocal appendicitis. SNUBH, Seoul National University Bundang Hospital.
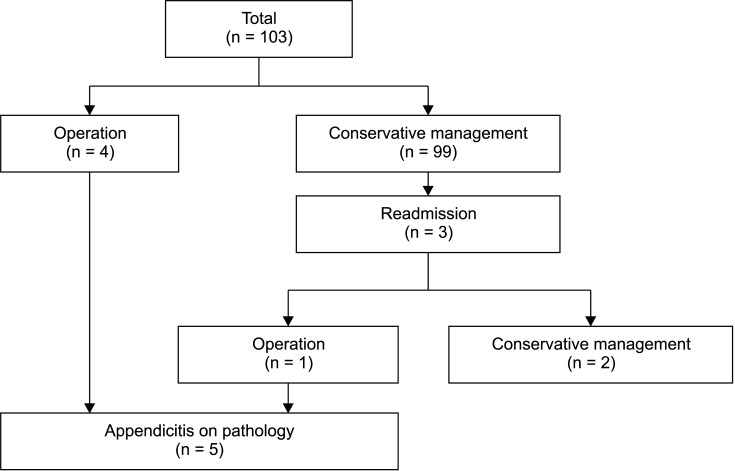
Fig. 5 Clinical course of patients with appendicitis CT score 2.
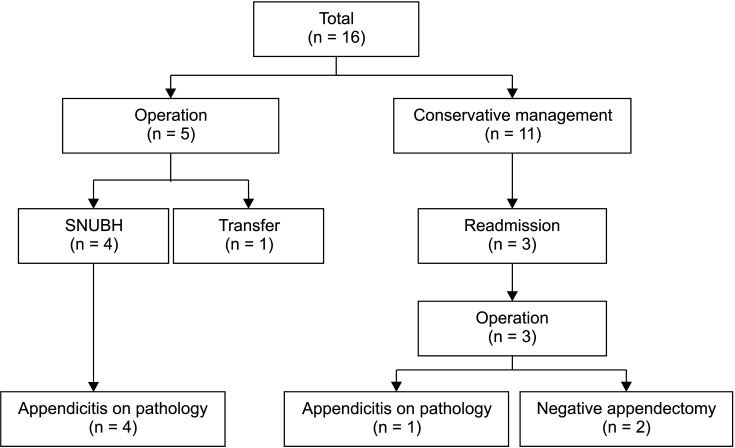
Fig. 6 Clinical course of patients with appendicitis CT score 3. SNUBH, Seoul National University Bundang Hospital.
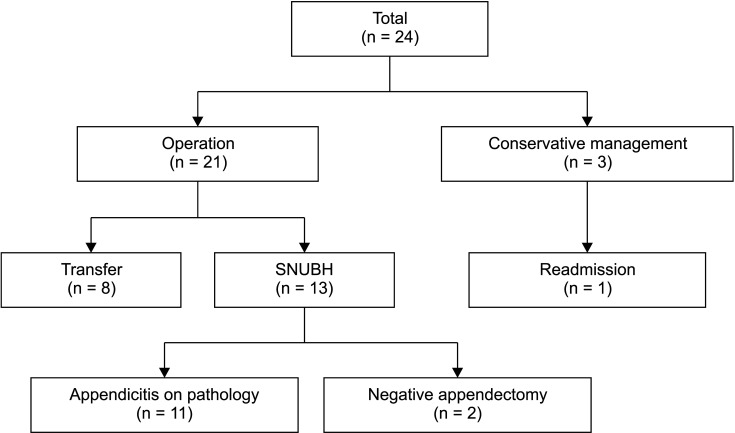
Fig. 7 Clinical course of patients with appendicitis CT score 4. SNUBH, Seoul National University Bundang Hospital.
Reference
-
1. Thompson AC, Olcott EW, Poullos PD, Jeffrey RB, Thompson MO, Rosenberg J, et al. Predictors of appendicitis on computed tomography among cases with borderline appendix size. Emerg Radiol. 2015; 22:385–394. PMID: 25687166.2. Fujishiro J, Watanabe E, Hirahara N, Terui K, Tomita H, Ishimaru T, et al. Laparoscopic versus open appendectomy for acute appendicitis in children: a nationwide retrospective study on postoperative outcomes. J Gastrointest Surg. 2021; 25:1036–1044. PMID: 32128682.3. Kosloske AM, Love CL, Rohrer JE, Goldthorn JF, Lacey SR. The diagnosis of appendicitis in children: outcomes of a strategy based on pediatric surgical evaluation. Pediatrics. 2004; 113(1 Pt 1):29–34. PMID: 14702443.4. Luo CC, Chien WK, Huang CS, Lo HC, Wu SM, Huang HC, et al. Trends in diagnostic approaches for pediatric appendicitis: nationwide population-based study. BMC Pediatr. 2017; 17:188. PMID: 29100501.5. Ramarajan N, Krishnamoorthi R, Gharahbaghian L, Pirrotta E, Barth RA, Wang NE. Clinical correlation needed: what do emergency physicians do after an equivocal ultrasound for pediatric acute appendicitis? J Clin Ultrasound. 2014; 42:385–394. PMID: 24700515.6. Nance ML, Adamson WT, Hedrick HL. Appendicitis in the young child: a continuing diagnostic challenge. Pediatr Emerg Care. 2000; 16:160–162. PMID: 10888451.7. Benabbas R, Hanna M, Shah J, Sinert R. Diagnostic accuracy of history, physical examination, laboratory tests, and point-of-care ultrasound for pediatric acute appendicitis in the emergency department: a systematic review and meta-analysis. Acad Emerg Med. 2017; 24:523–551. PMID: 28214369.8. Jaremko JL, Crockett A, Rucker D, Magnus KG. Incidence and significance of inconclusive results in ultrasound for appendicitis in children and teenagers. Can Assoc Radiol J. 2011; 62:197–202. PMID: 20493658.9. Debnath J, Kumar R, Mathur A, Sharma P, Kumar N, Shridhar N, et al. On the role of ultrasonography and CT scan in the diagnosis of acute appendicitis. Indian J Surg. 2015; 77(Suppl 2):221–226. PMID: 26729997.10. Partain KN, Patel A, Travers C, McCracken CE, Loewen J, Braithwaite K, et al. Secondary signs may improve the diagnostic accuracy of equivocal ultrasounds for suspected appendicitis in children. J Pediatr Surg. 2016; 51:1655–1660. PMID: 27039121.11. Yi DY, Lee KH, Park SB, Kim JT, Lee NM, Kim H, et al. Accuracy of low dose CT in the diagnosis of appendicitis in childhood and comparison with USG and standard dose CT. J Pediatr (Rio J). 2017; 93:625–631. PMID: 28445687.12. Yoon HM, Suh CH, Cho YA, Kim JR, Lee JS, Jung AY, et al. The diagnostic performance of reduced-dose CT for suspected appendicitis in paediatric and adult patients: a systematic review and diagnostic meta-analysis. Eur Radiol. 2018; 28:2537–2548. PMID: 29327290.13. Sim JY, Kim HJ, Yeon JW, Suh BS, Kim KH, Ha YR, et al. Added value of ultrasound re-evaluation for patients with equivocal CT findings of acute appendicitis: a preliminary study. Eur Radiol. 2013; 23:1882–1890. PMID: 23392792.14. Jang KM, Lee K, Kim MJ, Yoon HS, Jeon EY, Koh SH, et al. What is the complementary role of ultrasound evaluation in the diagnosis of acute appendicitis after CT? Eur J Radiol. 2010; 74:71–76. PMID: 19144480.15. Cavuşoğlu YH, Erdoğan D, Karaman A, Aslan MK, Karaman I, Tütün OC. Do not rush into operating and just observe actively if you are not sure about the diagnosis of appendicitis. Pediatr Surg Int. 2009; 25:277–282. PMID: 19184052.16. Kim K, Kim YH, Kim SY, Kim S, Lee YJ, Kim KP, et al. Low-dose abdominal CT for evaluating suspected appendicitis. N Engl J Med. 2012; 366:1596–1605. PMID: 22533576.17. Taylor GA, Callahan MJ, Rodriguez D, Smink DS. CT for suspected appendicitis in children: an analysis of diagnostic errors. Pediatr Radiol. 2006; 36:331–337. PMID: 16463152.18. Song B, Moon SB, Chae G, Park SB, Hong SK, Kim YH, et al. CT findings that indicate pediatric appendicitis: lessons from negative appendectomies. Adv Pediatr Surg. 2021; 27:15–21.19. Keating EM, Orth RC, Bisset GS, Starke HE, Cruz AT. Utility of computed tomography overreading and abdominal ultrasound in children with suspected appendicitis and nondiagnostic computed tomography at community hospitals. Pediatr Emerg Care. 2020; 36:564–570. PMID: 33136834.20. Kim M, Kim SJ, Cho HJ. Effect of surgical timing and outcomes for appendicitis severity. Ann Surg Treat Res. 2016; 91:85–89. PMID: 27478814.21. Podda M, Cillara N, Di Saverio S, Lai A, Feroci F, Luridiana G, et al. Antibiotics-first strategy for uncomplicated acute appendicitis in adults is associated with increased rates of peritonitis at surgery: a systematic review with meta-analysis of randomized controlled trials comparing appendectomy and non-operative management with antibiotics. Surgeon. 2017; 15:303–314. PMID: 28284517.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Can clinical scoring systems improve the diagnostic accuracy in patients with suspected adult appendicitis and equivocal preoperative computed tomography findings?
- The Usefulness of Computed Tomography for Patients with Equivocal Acute Appendicitis
- The Role of Computed Tomography in the Diagnosis of Acute Appendicitis
- Useful Ultrasound Findings of Pediatric Patients with Equivocal Results of Appendicitis: Analysis Based on a Structured Report Form
- Improving the value of ultrasound in children with suspected appendicitis: a prospective study integrating secondary sonographic signs
