Carotid cavernous fistula: Redefining the angioarchitecture
- Affiliations
-
- 1Fellow Skull Based Surgeon, PGIMER Chandigarh, Haryana, India
- 2Department of Neurosurgery, Pt. B. D. Sharma, PGIMS Rohtak. Haryana, India
- 3Department of Community Medicine, Pt. B. D. Sharma, PGIMS Rohtak. Haryana, India
- 4Department of Neurosurgery, SMS Medical College and Hospital, Jaipur, Rajasthan, India
- 5Department of Neurology, SMS Medical College and Hospital, Jaipur, Rajasthan, India
- KMID: 2537320
- DOI: http://doi.org/10.7461/jcen.2022.E2022.05.004
Abstract
Objective
Numerous classification schemes have been used for carotid cavernous fistula (CCF), each describing some aspect of the disease process but none of them provides a complete description of the fistula including its clinical features, natural history, arterial and venous architecture.
Methods
Retrospective clinical and radiological review was done for all the patients diagnosed with CCF and treated at our institute. The CCF were classified according to the proposed API-ACE classification along with Barrow and Thomas classification.
Results
Overall 28 patients (M=21, F=7) were diagnosed and treated during the 6-year period. 89.2% of CCF developed following an episode of head injury. Orbital symptoms were the most common presenting complaints. Barrows type A was the most predominant subtype (n=24) and most of the patients (n=23) demonstrated decreased ipsilateral carotid filling. Combined anterior and posterior drainage pattern was the most common drainage pattern and anterior drainage was more commonly observed than posterior drainage.
Conclusions
API-ACE classification helps to better understand and classify the angioarchitecture of CCF which could help better understand the clinical manifestations and guide in appropriate endovascular approach selection for treatment.
Figure
-

Fig. 1. (A) Angiogram in a post-traumatic CCF case showing communication of cavernous sinus with right ICA (high flow, direct) and right ECA. (B) Left ICA angiogram showing two sites of fistulous communication with cavernous sinus. CCF, carotid cavernous fistula; ICA, internal carotid artery; ECA, external carotid artery
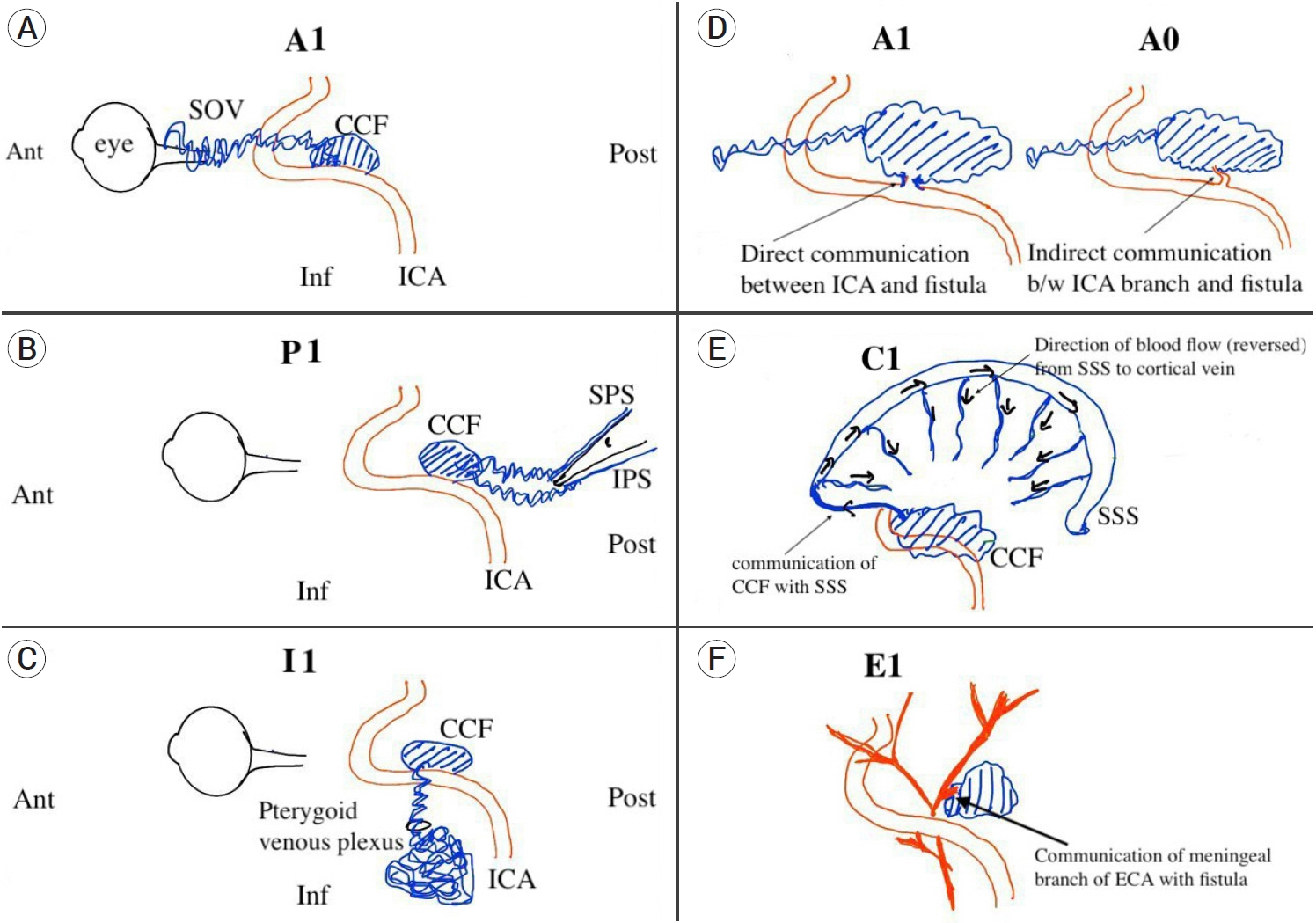
Fig. 2. Diagrammatic representation of components of API-ACE classification scheme. (A) Sketch showing CCF in relation to ICA with predominantly anterior drainage (A1) into the superior ophthalmic vein (SOV). (B) CCF with predominantly posterior drainage (P1) into the superior and inferior petrosal sinus (SPS and IPS) in relation to the petrous bone. (C) CCF with inferior venous drainage (I1) into the pterygoid venous plexus through foramen in the skull base. (D) Arterial communication with the ICA A1- direct communication with ICA; A0- arterial communication via a branch of ICA. (E) CCF causing venous hypertension and reversal of blood flow in the cortical vein via superior sagittal and spheno-petrosal sinus (C1). (F) CCF arising from meningeal branch of external carotid artery (E1). CCF, carotid cavernous fistula; ICA, internal carotid artery

Fig. 3. Schematic representation of API-ACE classification scheme and the distribution of cases in our series. ICA, internal carotid artery; ECA, external carotid artery

Fig. 4. Direct, high flow CCF with no ECA contribution, with both anterior and posterior ± inferior drainage pattern. (A) Right ICA lateral angiogram showing API- A1 C0 E0 (B) Right ICA lateral angiogram showing API- A1 C1 E0. CCF, carotid cavernous fistula; ECA, external carotid artery; ICA, internal carotid artery

Fig. 5. (A) Direct, high flow CCF with no ECA contribution, with predominant posterior venous drainage. Left ICA lateral angiogram showing PI- A1 C1 E0. (B) Direct, high flow CCF with no ECA contribution, with anterior venous drainage. Right ICA angiogram demonstrating A- A1 C0 E0 type of CCF. CCF, carotid cavernous fistula; ECA, external carotid artery; ICA, internal carotid artery
Reference
-
1. Abecassis IJ, Morton RP, Kim LJ, Ghodke BV, Levitt MR. Combined direct and indirect traumatic carotid-cavernous fistula (CCF): case report and review of the literature. J Clin Neurosci. 2017; Oct. 44:240–42.
Article2. Alam MS, Jain M, Mukherjee B, Sharma T, Halbe S, Jaisankar D, et al. Visual impairment in high flow and low flow carotid cavernous fistula. Sci Rep. 2019; 9(1):12872.
Article3. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985; Feb. 62(2):248–56.
Article4. Borden JA, Wu JK, Shucart WA. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg. 1995; Feb. 82(2):166–79.
Article5. Chi CT, Nguyen D, Duc VT, Chau HH, Son VT. Direct traumatic carotid cavernous fistula: angiographic classification and treatment strategies. Study of 172 cases. Interv Neuroradiol. 2014; Jul-Aug. 20(4):461–75.
Article6. Cognard C, Gobin YP, Pierot L, Bailly AL, Houdart E, Casasco A, et al. Cerebral dural arteriovenous fistulas: clinical and angiographic correlation with a revised classification of venous drainage. Radiology. 1995; Mar. 194(3):671–80.
Article7. Debrun GM. Angiographic workup of a carotid cavernous sinus fistula (CCF) or what information does the interventionalist need for treatment? Surg Neurol. 1995; Jul. 44(1):75–9.
Article8. Francis PM, Khayata MH, Zabramski JM, Spetzler RF. Carotid cavernous fistulae. Part 1: Presentation and features, in Carter LP, Spetzler RF (ed.) Neurovascular Surgery. New York: McGraw-Hill 1995. p. 1049-59.9. Jung KH, Kwon BJ, Chu K, Noh Y, Lee ST, Cho YD, et al. Clinical and angiographic factors related to the prognosis of cavernous sinus dural arteriovenous fistula. Neuroradiology. 2011; 53(12):983–92.
Article10. Leone G, Renieri L, Enriquez-Marulanda A, Dmytriw AA, Nappini S, Laiso A, et al. Carotid cavernous fistulas and dural arteriovenous fistulas of the cavernous sinus: validation of a new classification according to venous drainage. World Neurosurg. 2019; Aug. 128:e621–31.
Article11. Malan J, Lefeuvre D, Mngomezulu V, Taylor A. Angioarchitecture and treatment modalities in posttraumatic carotid cavernous fistulae. Interv Neuroradiol. 2012; Jun. 18(2):178–86.
Article12. Ringer AJ, Salud L, Tomsick TA. Carotid cavernous fistulas: anatomy, classification, and treatment. Neurosurg Clin N Am. 2005; Apr. 16(2):279–95. viii.
Article13. Thomas AJ, Chua M, Fusco M, Ogilvy CS, Tubbs RS, Harrigan MR, et al. Proposal of venous drainage-based classification system for carotid cavernous fistulae with validity assessment in a multicenter cohort. Neurosurgery. 2015; Sep. 77(3):380–5. discussion 385.
Article14. Winn HR. Youmans and Winn Neurological Surgery. Philadelpia: Elsevier;2017. p. 3525–29.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bilateral Traumatic Carotid-Cavernous Fistula
- Traumatic Carotid-cavernous Fistula Bringing about Intracerebral Hemorrhage
- A Case of Dural Carotid-Cavernous Sinus Fistula Associated with Ophthalmic Manifestations
- Dural Carotid-Cavernous Sinus Fistula
- A Case of Spontaneous of Traumatic Carotid Cavernous Fistula After Carotid Angiography
