Isolated primary hydatid cyst of the pancreas: Management challenges of a cystic masquerade
- Affiliations
-
- 1Department of Surgical Gastroenterology, All India Institute of Medical Sciences (AIIMS), Bhopal, Madhya Pradesh, India
- 2Department of Radiodiagnosis, All India Institute of Medical Sciences (AIIMS), Bhopal, Madhya Pradesh, India
- 3Departments of Pathology and Laboratory Medicine, All India Institute of Medical Sciences (AIIMS), Bhopal, Madhya Pradesh, India
- KMID: 2536391
- DOI: http://doi.org/10.14701/ahbps.22-031
Abstract
- Abdominal hydatid cyst disease mostly involves the liver. Involvement of the pancreas as an isolated primary organ is rare accounting for < 2% of all systemic echinococcosis cases. It mostly involves the head of the pancreas. Symptoms depend on the location, size, and associated complications; therefore, it can have varied presentations including acute pancreatitis. On imaging, it can mimic other common pancreatic cystic lesions like pseudocyst or cystic neoplasm. Accurate preoperative diagnosis is usually difficult and requires a very high index of suspicion even in endemic areas. Herein, a case of primary isolated hydatid cyst of the pancreas that was initially diagnosed and managed as acute pancreatic pseudocyst is reported.
Figure
-

Fig. 1 (A) Coronal contrast-enhanced computed tomography (CT) image (axial view) showing a well-defined round unilocular cystic lesion in the head of the pancreas with a well-defined peripherally enhancing margin without any solid enhancing tissue or septations. (B) Contrast-enhanced CT image (coronal view) showing a well-defined round unilocular cystic lesion in the head of the pancreas with a well-defined peripherally enhancing margin without any internal solid component or septations. (C) Coronal T2W magnetic resonance imaging showing a well-defined smooth-walled unilocular cystic lesion in the head of the pancreas. (D) Magnetic resonance cholangiopancreatography image showing a large and well defined cystic lesion at the region of pancreatic head. The extrahepatic bile duct is seen separately without any evidence of bile duct dilatation.
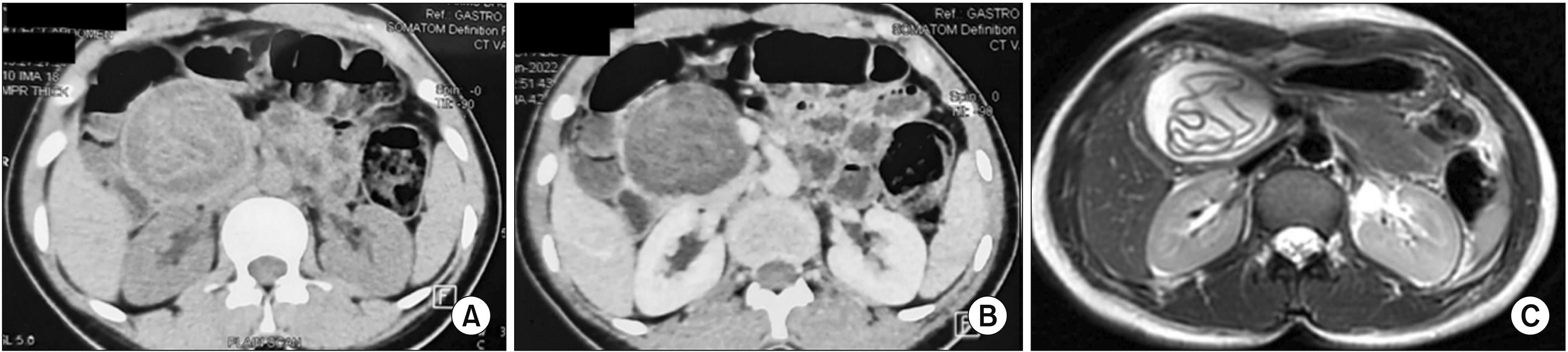
Fig. 2 (A) Plain computed tomography (CT) scan (axial view) showing a round well-defined cystic lesion in the head of the pancreas with multiple internal floating membranes. (B) Contrast-enhanced CT scan (axial view) showing a round well-defined hypodense cystic lesion in the head of the pancreas with multiple internal hyperdense floating membranes. (C) T2W magnetic resonance imaging image (axial view) showing the characteristic appearance of hydatid cyst as a well-defined cystic lesion with multiple floating membranes within (water Lilly sign).

Fig. 3 Port positions (marked with 'X') used in the laparoscopic partial cystopericystectomy procedure. Two 10 mm ports (at the umbilicus [marked with *] for the camera, second for surgeon’s left working hand/suction/specimen extraction), two 5 mm ports (lower one for surgeon’s right working hand and upper one for assistant/surgeon).

Fig. 4 (A) Intraoperative image showing a large cystic lesion (*) in the head of the pancreas. (B) Cyst exposure after the division of overlying gastrocolic omentum. The cyst has been isolated from the surrounding structures by roller gauze soaked in scolicidal agent (10% Povidone-iodine). (C) Cyst content is being aspirated in a controlled manner. (D) Cyst is being opened with an ultrasonic energy device in a controlled manner with 2 suction cannulas placed close by to contain spillage. (E) Cyst contents (* membrane) are being evacuated with a 10 mm suction cannula. (F) Partial cystopericystectomy is being performed using ultrasonic energy device. (G) Opened up cyst after partial cystopericystectomy. (H) Omentoplasty.

Fig. 5 Evacuated hydatid cyst membranes.
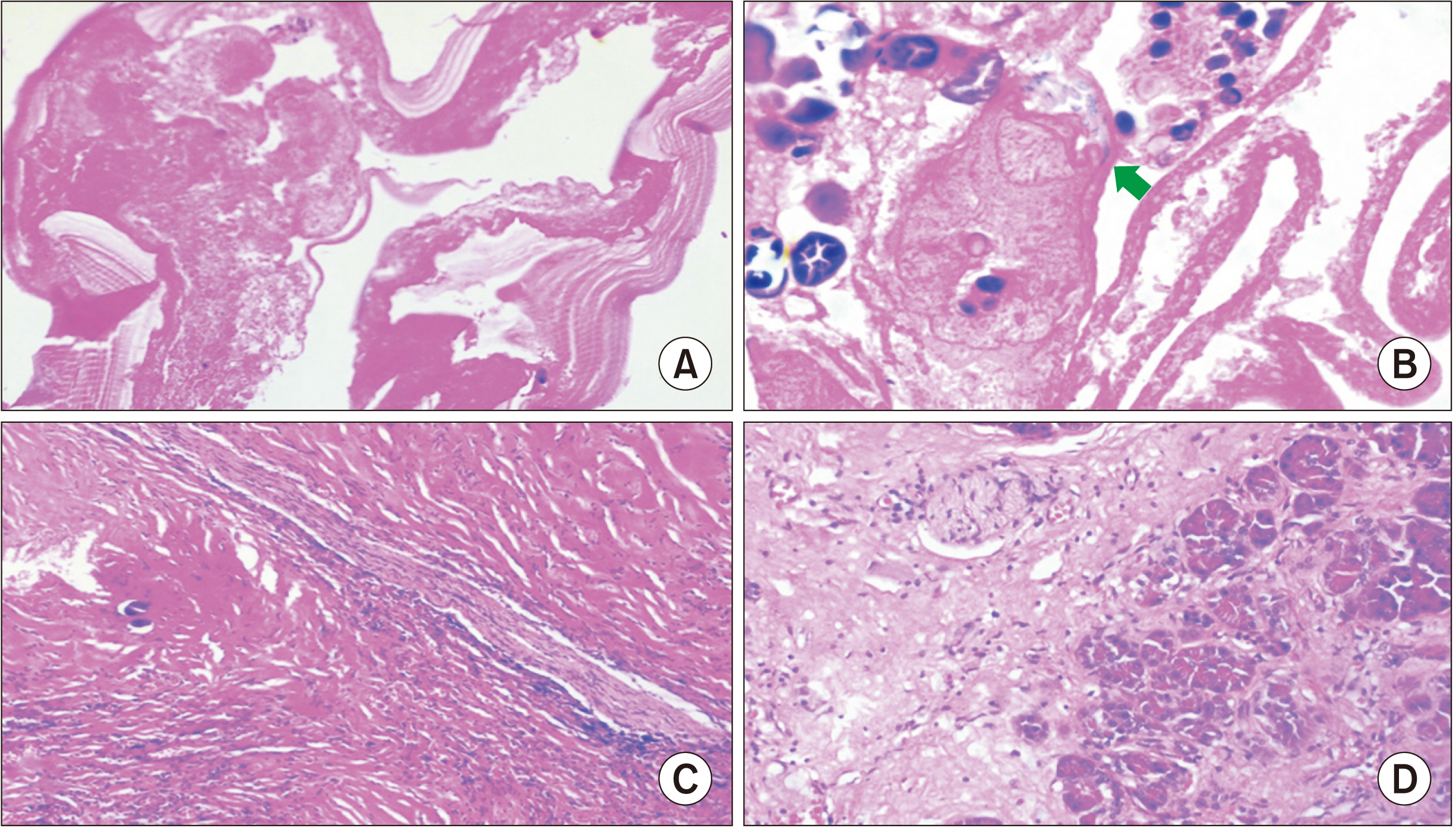
Fig. 6 (A) Hydatid cyst wall showing lamellated membrane with inner degenerative germinal layer (H&E, low power 200×). (B) The degenerative protoscolices of echinococcus with hooklets (arrow) (H&E, high power 400×). (C) Pericyst (H&E, low power 200×). (D) Adjoining pancreas showing chronic pancreatitis changes with acinar atrophy and interstitial fibrosis (H&E, low power 200×).
Reference
-
1. Akbulut S, Yavuz R, Sogutcu N, Kaya B, Hatipoglu S, Senol A, et al. 2014; Hydatid cyst of the pancreas: report of an undiagnosed case of pancreatic hydatid cyst and brief literature review. World J Gastrointest Surg. 6:190–200. DOI: 10.4240/wjgs.v6.i10.190. PMID: 25346801. PMCID: PMC4208043.2. Ahmed Z, Chhabra S, Massey A, Vij V, Yadav R, Bugalia R, et al. 2016; Primary hydatid cyst of pancreas: case report and review of literature. Int J Surg Case Rep. 27:74–77. DOI: 10.1016/j.ijscr.2016.07.054. PMID: 27552034. PMCID: PMC4995534.3. Wu Y, Gong J, Xiong W, Yu X, Lu X. 2021; Primary pancreatic hydatid cyst: a case report and literature review. BMC Gastroenterol. 21:164. DOI: 10.1186/s12876-021-01753-1. PMID: 33849455. PMCID: PMC8045313.4. Chinya A, Khanolkar A, Kumar J, Sinha SK. 2015; Isolated hydatid cyst of the pancreas masquerading as pancreatic pseudocyst. BMJ Case Rep. 2015:bcr2015211307. DOI: 10.1136/bcr-2015-211307. PMID: 26264949. PMCID: PMC4533679.5. Cankorkmaz L, Gümüş C, Celiksöz A, Köylüoğlu G. 2011; Primary hydatid disease of the pancreas mimicking pancreatic pseudo-cyst in a child: case report and review of the literature. Turkiye Parazitol Derg. 35:50–52. DOI: 10.5152/tpd.2011.13. PMID: 21618194.6. WHO Informal Working Group. 2003; International classification of ultrasound images in cystic echinococcosis for application in clinical and field epidemiological settings. Acta Trop. 85:253–261. DOI: 10.1016/S0001-706X(02)00223-1. PMID: 12606104.7. Stojkovic M, Rosenberger K, Kauczor HU, Junghanss T, Hosch W. 2012; Diagnosing and staging of cystic echinococcosis: how do CT and MRI perform in comparison to ultrasound? PLoS Negl Trop Dis. 6:e1880. DOI: 10.1371/journal.pntd.0001880. PMID: 23145199. PMCID: PMC3493391.8. Javed A, Agarwal G, Aravinda PS, Manipadam JM, Puri SK, Agarwal AK. 2020; Hydatid cyst of the pancreas: a diagnostic dilemma. Trop Gastroenterol. 41:73–81.9. Kısaoğlu A, Özoğul B, Atamanalp SS, Pirimoğlu B, Aydınlı B, Korkut E. 2015; Incidental isolated pancreatic hydatid cyst. Turkiye Parazitol Derg. 39:75–77. DOI: 10.5152/tpd.2015.3293. PMID: 25917590.10. Makni A, Jouini M, Kacem M, Safta ZB. 2012; Acute pancreatitis due to pancreatic hydatid cyst: a case report and review of the literature. World J Emerg Surg. 7:7. DOI: 10.1186/1749-7922-7-7. PMID: 22445170. PMCID: PMC3325852.11. Mandelia A, Wahal A, Solanki S, inivas M Sr, Bhatnagar V. 2012; Pancreatic hydatid cyst masquerading as a choledochal cyst. J Pediatr Surg. 47:e41–e44. DOI: 10.1016/j.jpedsurg.2012.07.054. PMID: 23164030.12. Ibis C, Albayrak D, Altan A. 2009; Primary hydatid disease of pancreas mimicking cystic neoplasm. South Med J. 102:529–530. DOI: 10.1097/SMJ.0b013e31819c3bef. PMID: 19373169.13. Dziri C, Dougaz W, Bouasker I. 2017; Surgery of the pancreatic cystic echinococcosis: systematic review. Transl Gastroenterol Hepatol. 2:105. DOI: 10.21037/tgh.2017.11.13. PMID: 29354762. PMCID: PMC5763016.14. Imam A, Khoury T, Weis D, Khalayleh H, Adeleh M, Khalaileh A. 2019; Laparoscopic cystectomy for pancreatic echinococcosis: a case report and literature review. Ann Hepatobiliary Pancreat Surg. 23:87–90. DOI: 10.14701/ahbps.2019.23.1.87. PMID: 30863816. PMCID: PMC6405372.15. Vasilescu A, Tarcoveanu E, Crumpei F, Blaj M, Bejan V, Bradea C. 2020; Laparoscopic approach of primary hydatid cyst of the pancreas - case report and literature review. Chirurgia (Bucur). 115:261–266. DOI: 10.21614/chirurgia.115.2.261. PMID: 32369731.16. Suryawanshi P, Khan AQ, Jatal S. 2011; Primary hydatid cyst of pancreas with acute pancreatitis. Int J Surg Case Rep. 2:122–124. DOI: 10.1016/j.ijscr.2011.02.011. PMID: 22096702. PMCID: PMC3199727.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- US and CT Findings of Splenic Hydatid Cyst: A Case Report
- Primary Giant Splenic and Hepatic Echinococcal Cysts Treated by Laparoscopy
- Laparoscopic management of giant hepatic hydatid cyst in a 12-year-old boy: a case report
- Overview of cystic lesion of the pancreas
- Pathologic Features of Pancreatic Cystic Neoplasms
