Functional reconstruction of the thumb by heterotopic thumb-to-thumb replantation and secondary opponensplasty in bilateral amputation in the upper extremities: a case report
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Gwangmyeong Sungae General Hospital, Gwangmyeong, Korea
- KMID: 2536216
- DOI: http://doi.org/10.12790/ahm.22.0042
Abstract
- In traumatic amputations in the upper extremities, replantation has been commonly attempted with high success rates. However, successful replantation implies both the maintenance of length and good functional outcomes of the restored hand. Since the thumb accounts for 40% to 50% of hand function, the utmost priority is on the salvage of the thumb. In cases when replantation is not feasible, various efforts have been made to replace the thumb, including pollicization of the index finger, toe transfer, lengthening of the thumb stump, and deepening of the first web space. Alternatively, heterotopic thumb-to-thumb replantation has been suggested as a rescue plan in rare circumstances of bilateral amputation in the upper extremities. However, even if heterotopic replantation is successful, there are situations in which a severe crushing injury to the thenar muscles of the recipient’s thumb causes opposition failure of the reconstructed thumb. We report a case of functional reconstruction of the thumb in a rare case of bilateral mangling amputations in the upper extremities, by a heterotopic thumb-to-thumb replantation combined with secondary opponensplasty to compensate for the opposition failure.
Figure
-
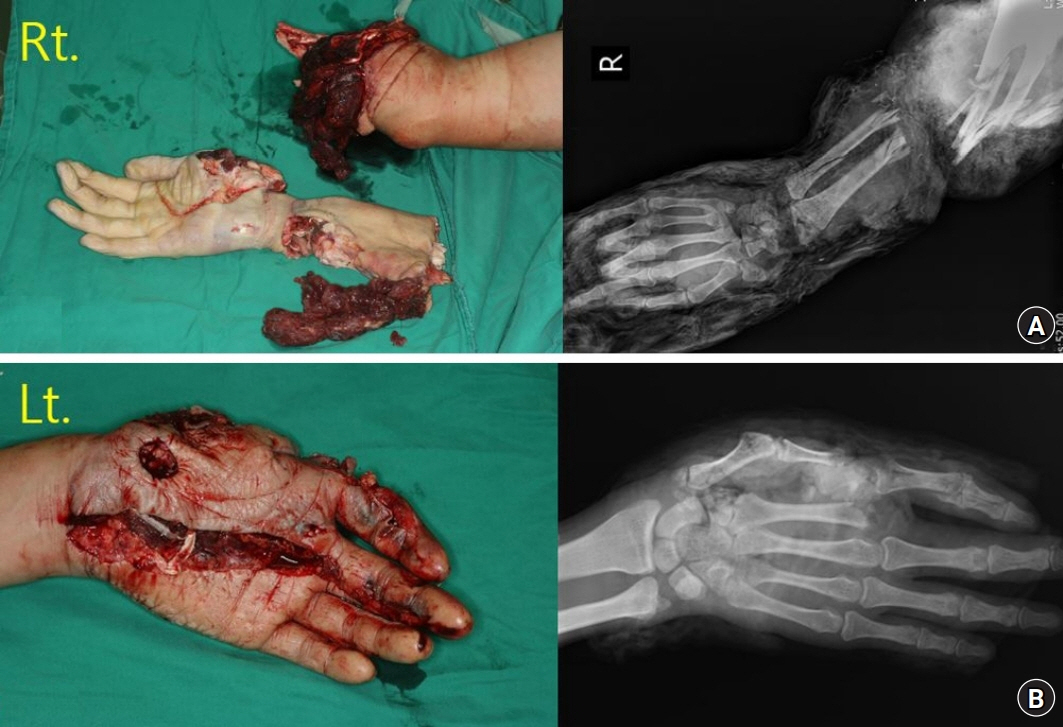
Fig. 1. Initial preoperative photo showing bilateral mangling amputations on the upper extremity. (A) The right forearm was completely amputated at proximal 1/3 level of the forearm with comminution on both ulna and radius. (B) The nondominant left hand had crushing on the thumb, index, middle finger, and palm. The left thumb was subtotally amputated without circulation and severe crushing was found on the thenar muscles; however, the index finger retained blood circulation on the fingertips. On plain radiography, the thumb was amputated at the 1st carpometacarpal joint and the index finger showed bony amputation at proximal phalangeal head level.
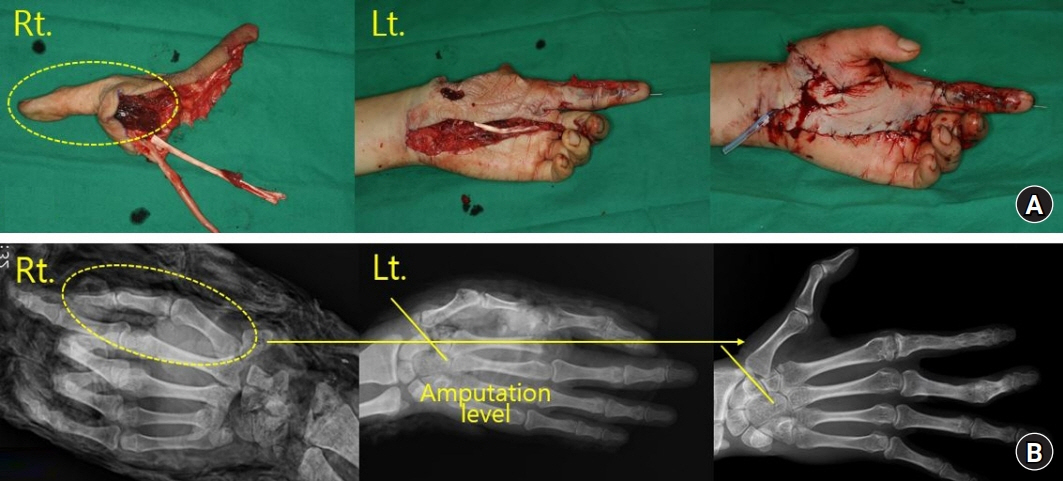
Fig. 2. Intraoperative photo showing the heterotopic thumb-to-thumb replantation. (A) The right thumb is harvested at the 1st carpometacarpal joint level and replanted to the left hand. (B) The plain radiography taken before thumb replantation and 2 years after surgery, showing the transferred right thumb to the left hand.

Fig. 3. Preoperative and intraoperative photo of extensor indicis proprius (EIP) opponensplasty. (A) Preoperative photo taken at 2-year follow-up after the initial thumb replantation, showing limitations in thumb opposition. (B) The EIP tendon was identified through a linear incision over the dorsal ulnar aspect of the 2nd metacarpophalangeal joint. The tendon was detached free from the extensor digitorum communis. (C) Through wide excision of the deep fascia of forearm, the distal part of the muscle belly is gently freed and pulled out. (D) The muscle-tendon unit was tunneled through the subcutaneous border of the ulna and brought out through another incision near the pisiform. (E) Due to the absence of an abductor pollicis brevis, EIP was inserted on the extensor pollicis longus (EPL) tendon. (F) EIP was connected to EPL tendon with a weaving suture using PDS 4-0 (Ethicon Inc., Raritan, NJ, USA).

Fig. 4. Follow-up photo of the 10th year after extensor indicis proprius (EIP) opponensplasty taken at the outpatient clinic. (A) Significant improvement in the opposition of thumb was seen, allowing the pinching on the ring and little fingers. (B) Follow-up photo of the 10th year after EIP opponensplasty taken at the outpatient clinic. (B) The radial abduction increased to 55°. (C) The palmar abduction increased to 60°. (D) The patient recovered satisfactory grip power to grab a bottle.
Reference
-
References
1. Tosti R, Treiser MD, Eberlin KR. Contralateral heterotopic thumb-to-thumb replantation with free ulnar forearm fasciocutaneous flap and targeted muscle reinnervation. J Hand Surg Am. 2020; 45:71. e1-5.
Article2. Reigstad A, Hetland KR. Cross thumb transfer. J Hand Surg Br. 1993; 18:778–80.
Article3. Anderson GA, Lee V, Sundararaj GD. Extensor indicis proprius opponensplasty. J Hand Surg Br. 1991; 16:334–8.
Article4. Kutz JE, Sinclair SW, Rao V, Carlier A. Cross-hand replantation: preliminary case report. J Microsurg. 1982; 3:251–4.
Article5. Tegtmeier RE. Thumb-to-thumb transfer following severe electrical burns to both hands. J Hand Surg Am. 1981; 6:269–71.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Thumb reconstruction with a double flap after thumb replantation failure using a reverse homodigital dorsoulnar flap and a cross-finger flap: a case report
- Thumb Tip Reconstruction with Subcutaneous Pocket Graft: 2 Cases Report
- Thumb Reconstruction with a Osteocutaneous Free Flap Transfer with Partial 1 st Matatarsus (Case Report )
- Pollicization: Two Cases report
- Free Toe-to-Thumb Transplantation with Microsurgical Technique
