Surgical outcomes of laparoscopic trachelectomy following supracervical hysterectomy: a multicenter study
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Tanta University, Tanta, Egypt
- 2Department of Pathology, Tanta University, Tanta, Egypt
- 3Department of GIT Surgery and Oncology, Tanta University, Tanta, Egypt
- 4Department of Obstetrics and Gynecology, Benha University, Benha, Egypt
- KMID: 2535962
- DOI: http://doi.org/10.5468/ogs.22094
Abstract
Objective
To evaluate the feasibility, safety, and surgical outcomes of laparoscopic trachelectomy after supracervical hysterectomy.
Methods
This multicenter study was conducted at Tanta University, Benha University, and Aminah Laparoscopy Center (Benha, Egypt) from June 1, 2018 to October 31, 2021. Forty patients were recruited for this study and counseled on laparoscopic trachelectomy to treat their symptoms after supracervical hysterectomy. Furthermore, cervical biopsy was performed to detect and exclude any malignancy. Histopathological examination of cervical specimens was performed after surgery. Operative details and outcomes were recorded.
Results
The median age of the patients was 42 years (range, 38-47). The median body mass index was 25 years (range, 22- 28). The median interval between hysterectomy and the clinical presentation was 4.40 years (range, 3.58-5.25). Most patients presented with abnormal vaginal discharge (40%) and bleeding (25%). Moreover, a cervical biopsy result revealed stump carcinoma in three cases (7.5%) that were excluded. The median operative time was 210 minutes (range, 170-220). The median blood loss was 270 mL (range, 220-320). Additionally, histopathological examinations revealed that chronic non-specific cervicitis was present in 54.05% of trachelectomy specimens. There were no significant differences between symptomatic and asymptomatic patients regarding operative outcomes, except adhesions, which were more significantly increased in symptomatic patients (P=0.015). Minimal complications, both operative and postoperative, were related to the procedure.
Conclusion
Although the operative time was long and adhesions were common during laparoscopic trachelectomy, the procedure was feasible and safe, with minimal complications.
Keyword
Figure
-
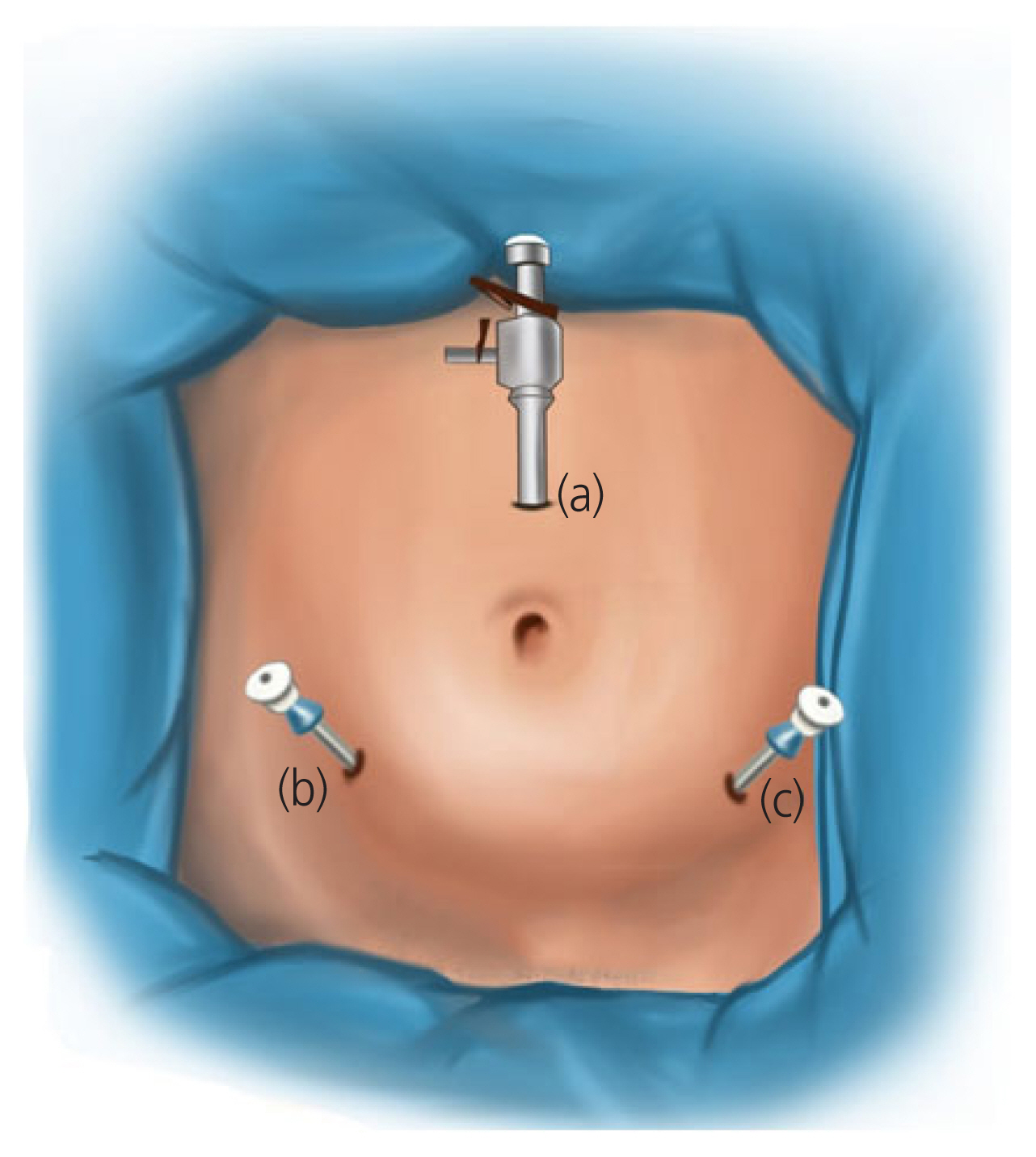
Fig. 1 Position of ports in laparoscopic trachelectomy (a) 10 mm port at Lee-Hwang point, (b) and (c) 5 mm port at midclavicular line, two fingers above the anterior superior iliac spines.
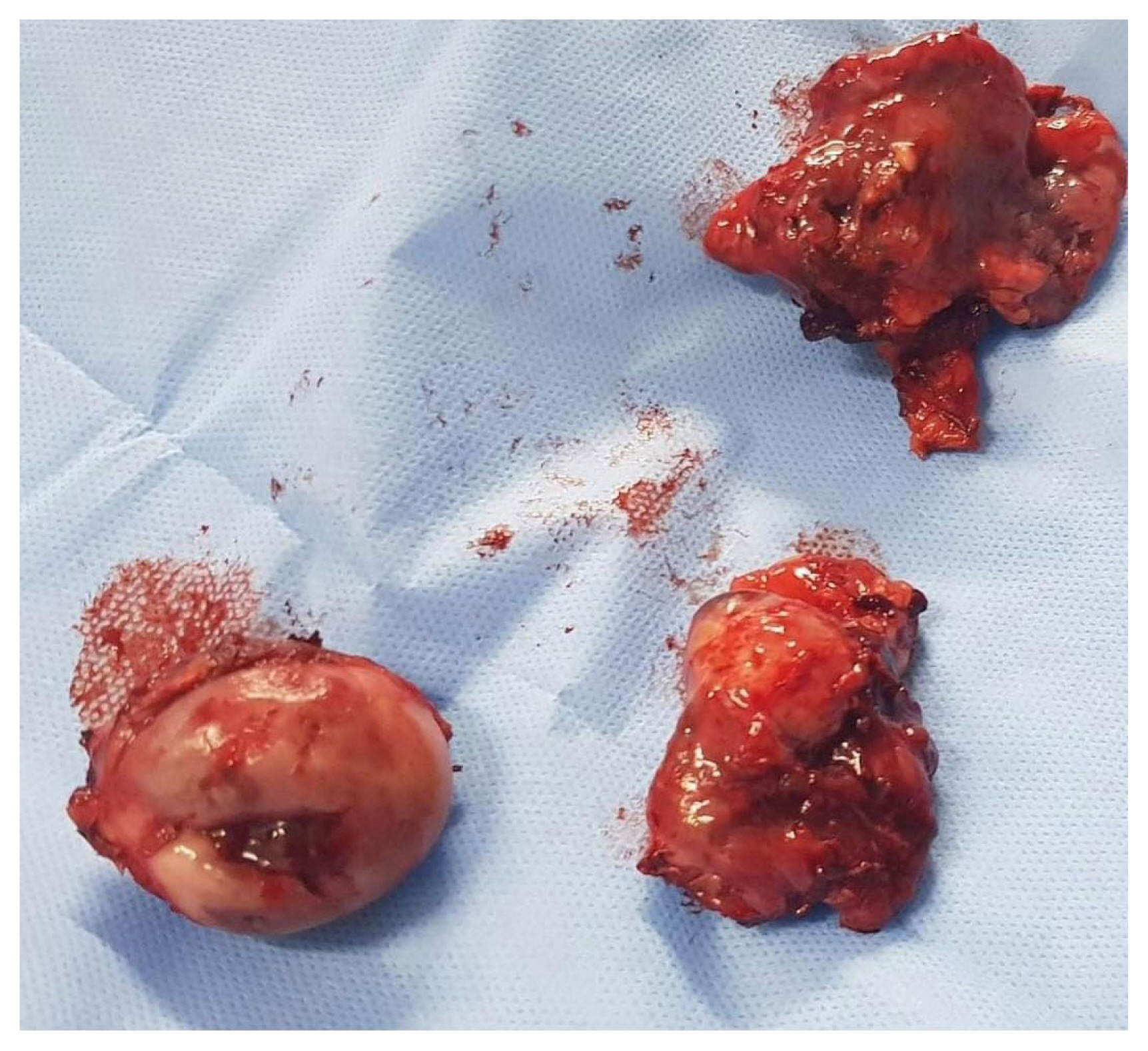
Fig. 2 Cervical stump and bilateral adnexa.

Fig. 3 (A) Adhesiolysis of omentum and bowel from lateral pelvic wall and cervical stump. (B) Douglas pouch free of adhesions. (C) Urinary bladder dissected downwards and colpotomizer pushed upwards to delineate the cervix. (D) Excision of the cervix by monopolar energy using hook.

Fig. 4 (A) Chronic nonspecific cervicitis; endocervical mucosa with lymphocytic inflammation (×100).(B) Cervical endometriosis; a focus within the cervical stroma containing endometrial glands and stroma (×200). (C) CIN I; nuclear hyperchromasia and pleomorphism involving the lower one third of epithelium (×400). (D) CIN II; nuclear hyperchromasia and pleomorphism involving the lower 2/3rd of the epithelium (×400). CIN, cervical intraepithelial neoplasia.
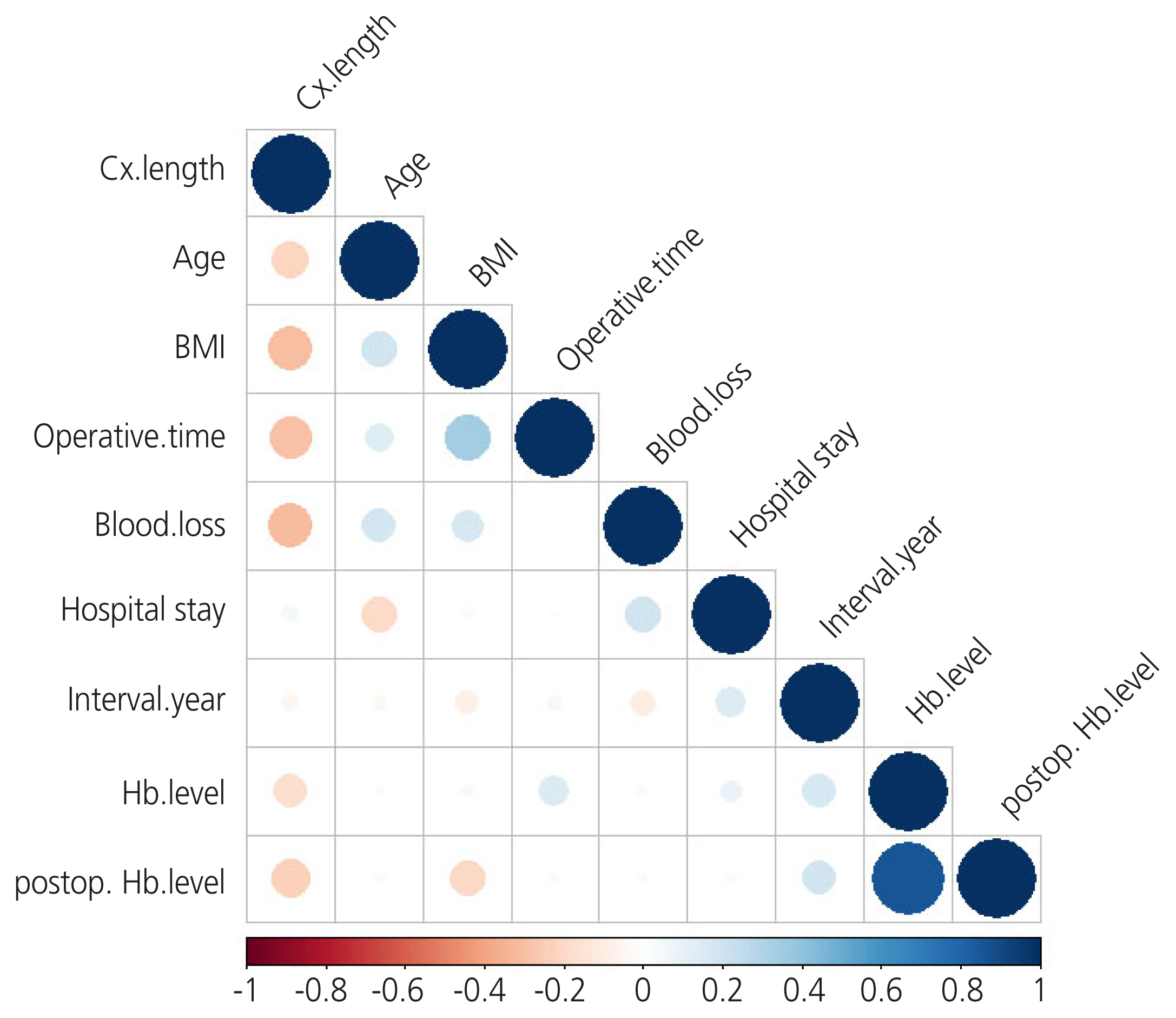
Fig. 5 Correlation matrix showing the correlation coefficients between other variables. Cx, cervical length; BMI, body mass index; Hb, hemoglobin.
Reference
-
References
1. Committee opinion No 701: choosing the route of hysterectomy for benign disease. Obstet Gynecol. 2017; 129:e155–9.2. Aarts JW, Nieboer TE, Johnson N, Tavender E, Garry R, Mol BW, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst Rev. 2015; 2015:CD003677.
Article3. Kives S, Lefebvre G; Clinical Gynaecology Committee. Supracervical hysterectomy. J Obstet Gynaecol Can. 2010; 32:62–8.4. Pegu B, Srinivas BH, Saranya TS, Murugesan R, Priyadarshini Thippeswamy S, Gaur BPS. Cervical polyp: evaluating the need of routine surgical intervention and its correlation with cervical smear cytology and endometrial pathology: a retrospective study. Obstet Gynecol Sci. 2020; 63:735–42.
Article5. Yuksel S, Tuna G, Celik HG, Salman S. Endometrial polyps: is the prediction of spontaneous regression possible? Obstet Gynecol Sci. 2021; 64:114–21.
Article6. Sasaki KJ, Cholkeri-Singh A, Sulo S, Miller CE. Persistent bleeding after laparoscopic supracervical hysterectomy. JSLS. 2014; 18:e2014-002064.
Article7. Scott JR, Sharp HT, Dodson MK, Norton PA, Warner HR. Subtotal hysterectomy in modern gynecology: a decision analysis. Am J Obstet Gynecol. 1997; 176:1186–91.
Article8. Neis F, Reisenauer C, Kraemer B, Wagner P, Brucker S. Retrospective analysis of secondary resection of the cervical stump after subtotal hysterectomy: why and when? Arch Gynecol Obstet. 2021; 304:1519–26.
Article9. Hellström AC, Hellman K, Pettersson BF, Andersson S. Carcinoma of the cervical stump: fifty years of experience. Oncol Rep. 2011; 25:1651–4.
Article10. Shen Z, Zhou Y, Cheng Y, Li M, Wu D. Retrospective analysis of surgery for cervical stump carcinoma at early stage. Mol Clin Oncol. 2018; 8:352–5.
Article11. Asnafi N, Basirat Z, Hajian-Tilaki KO. Outcomes of total versus subtotal abdominal hysterectomy. East Mediterr Health J. 2010; 16:176–9.
Article12. Elbohoty SB, Dawood AS, Elgergawy AE. Gynecological presentations following supravaginal hysterectomy for benign pathologies. W J Gynecol Women’s Health. 2020; 3:WJGWH.MS.ID.000558.13. Tsafrir Z, Aoun J, Papalekas E, Taylor A, Schiff L, Theoharis E, et al. Risk factors for trachelectomy following supracervical hysterectomy. Acta Obstet Gynecol Scand. 2017; 96:421–5.
Article14. Andersen LL, Zobbe V, Ottesen B, Gluud C, Tabor A, Gimbel H, et al. Five-year follow up of a randomised controlled trial comparing subtotal with total abdominal hysterectomy. BJOG. 2015; 122:851–7.
Article15. Okaro EO, Jones KD, Sutton C. Long term outcome following laparoscopic supracervical hysterectomy. BJOG. 2001; 108:1017–20.
Article16. Lieng M, Qvigstad E, Istre O, Langebrekke A, Ballard K. Long-term outcomes following laparoscopic supracervical hysterectomy. BJOG. 2008; 115:1605–10.
Article17. Dawood AS, Harras H, Lotfy HA. Histopathological findings in symptomatizing patients after supracervical hysterectomy: a cross sectional study. W J Gynecol Women’s Health. 2021; 5:WJGWH.MS.ID.000601.
Article18. Nezhat CH, Nezhat F, Roemisch M, Seidman DS, Nezhat C. Laparoscopic trachelectomy for persistent pelvic pain and endometriosis after supracervical hysterectomy. Fertil Steril. 1996; 66:925–8.
Article19. Vieira MA, Rendón GJ, Munsell M, Echeverri L, Frumovitz M, Schmeler KM, et al. Radical trachelectomy in early-stage cervical cancer: a comparison of laparotomy and minimally invasive surgery. Gynecol Oncol. 2015; 138:585–9.
Article20. Lu Z, Guo C, Wang T, Qiu J, Hua K. Characteristics, complications, and outcomes of early-stage cervical stump carcinoma: laparoscopy versus laparotomy. J Int Med Res. 2021; 49:300060521992247.
Article21. Yunker A, Curlin H, Banet N, Fadare O, Steege J. Does the uterine cervix become abnormally reinnervated after subtotal hysterectomy and what is the association with future trachelectomy? J Minim Invasive Gynecol. 2015; 22:261–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Incidence of cyclical bleeding after laparoscopic supracervical hysterectomy
- Update in Laparoscopic Hysterectomy and Laparoscopic Myomectomy
- Comparative study of laparoscopic assisted vaginal hysterectomy and laparoscopic supracervical hysterectomy
- Prevotella bivia Infection Following Supracervical Hysterectomy: Case Report with a Review of Literatures
- A case of treatment by embolization of uterine arterial pseudoaneurysm following laparoscopic supracervical hysterectomy
