Adult-onset Leigh syndrome due to m.9176T>C mutation with cortical involvement
- Affiliations
-
- 1Department of Neurology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 2Department of Neurology, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea
- KMID: 2535729
- DOI: http://doi.org/10.14253/acn.2022.24.2.107
Abstract
- We describe the case of a 22-year-old female complaining of ophthalmoplegia, which deteriorated with seizure. Leigh syndrome (LS) was diagnosed by identifying the m.9176T>C mutation. She improved with vitamin cocktail therapy plus intravenous methylprednisolone, and had an excellent prognosis. This was the first case of an adult patient with LS presenting with the m.9176T>C mutation and reporting cortical symptoms, which in this case comprised cortical vision loss, and cortical, basal ganglia, and brainstem signal changes on magnetic resonance imaging.
Figure
-

Fig. 1. Pedigree of the patient. The patient had two older brothers, both of whom had complained of diplopia or gait disturbance. The older brother complained of diplopia at 12 years old and gait disturbance during his 20s, but recovered spontaneously and survived. The younger brother died when he was 5 years old, a few weeks after gait disturbance had been observed. No family member other than the patient received genetic testing. Pt, patient.
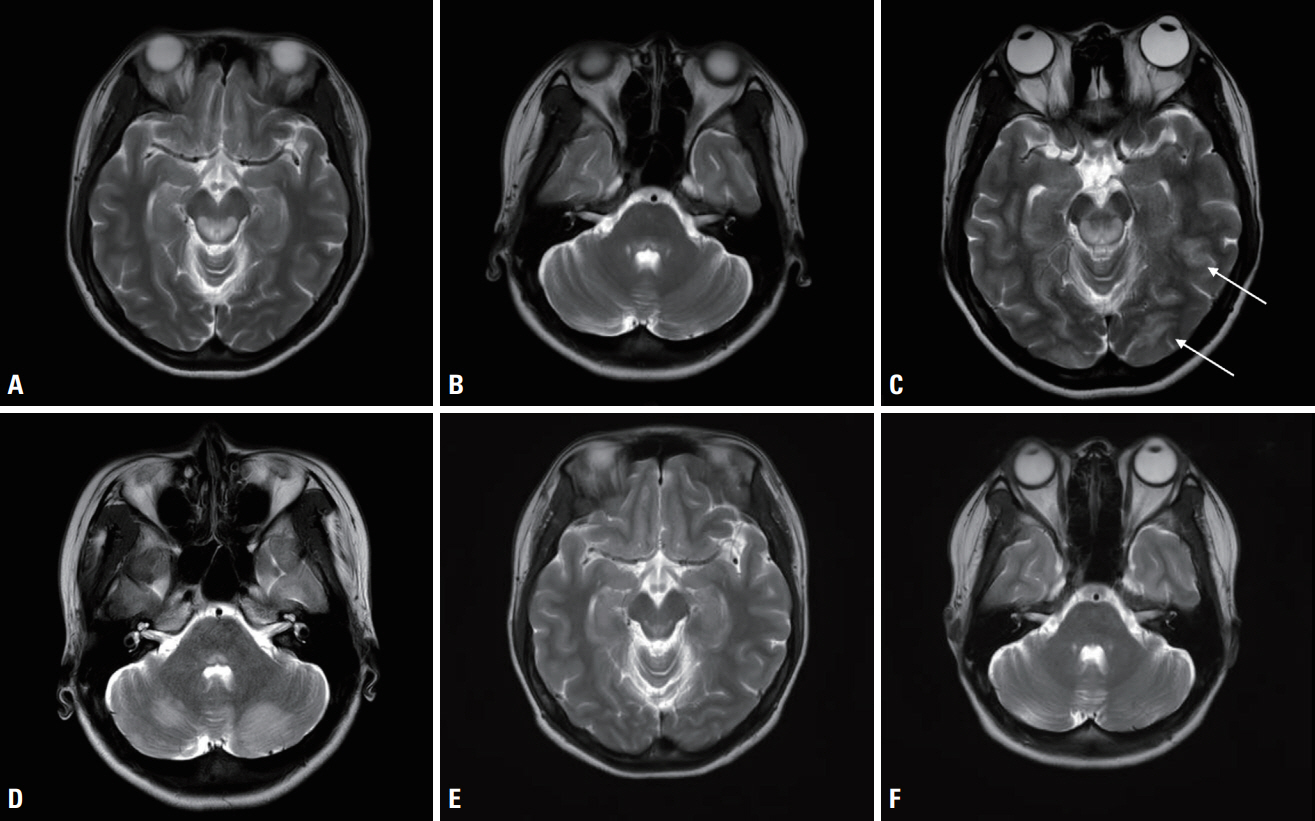
Fig. 2. (A) An axial T2-weighted image obtained on admission showed a high signal intensity (SI) in the dorsal midbrain, but no signal change in the cortex (B) or in the cerebellum. (C) An axial T2-weighted image obtained after aggravation showed a high SI in the bilateral occipital cortex (arrows). (D) In an axial T2-weighted image obtained after aggravation, a high SI also presented in the bilateral cerebellum. (E) An axial T2-weighted image obtained 16 months after discharge revealed a decrease in the extent of the high SIs in the dorsal midbrain, occipital cortex, and (F) bilateral cerebellum.
Reference
-
1. Rahman S, Blok RB, Dahl HH, Danks DM, Kirby DM, Chow CW, et al. Leigh syndrome: clinical features and biochemical and DNA abnormalities. Ann Neurol. 1996; 39:343–351.2. McKelvie P, Infeld B, Marotta R, Chin J, Thorburn D, Collins S. Lateadult onset Leigh syndrome. J Clin Neurosci. 2012; 19:195–202.3. Campos Y, Martín MA, Rubio JC, Solana LG, García-Benayas C, Terradas JL, et al. Leigh syndrome associated with the T9176C mutation in the ATPase 6 gene of mitochondrial DNA. Neurology. 1997; 49:595–597.4. Makino M, Horai S, Goto Y, Nonaka I. Confirmation that a T-to-C mutation at 9176 in mitochondrial DNA is an additional candidate mutation for Leigh’s syndrome. Neuromuscul Disord. 1998; 8:149–151.5. Ichikawa K, Tsuyusaki Y, Shimbo H, Goto T. Late-onset Leigh syndrome with m.9176T>C mutation in the mitochondrial ATPase 6 gene. Pediatr Int. 2019; 61:1055–1056.6. Ronchi D, Bordoni A, Cosi A, Rizzuti M, Fassone E, Di Fonzo A, et al. Unusual adult-onset Leigh syndrome presentation due to the mitochondrial m.9176T>C mutation. Biochem Biophys Res Commun. 2011; 412:245–248.7. Lake NJ, Compton AG, Rahman S, Thorburn DR. Leigh syndrome: one disorder, more than 75 monogenic causes. Ann Neurol. 2016; 79:190–203.8. Wei Y, Cui L, Peng B. Mitochondrial DNA mutations in late-onset Leigh syndrome. J Neurol. 2018; 265:2388–2395.9. Barcelos I, Shadiack E, Ganetzky RD, Falk MJ. Mitochondrial medicine therapies: rationale, evidence, and dosing guidelines. Curr Opin Pediatr. 2020; 32:707–718.10. Chuquilin M, Govindarajan R, Peck D, Font-Montgomery E. Response to immunotherapy in a patient with adult onset Leigh syndrome and T9176C mtDNA mutation. Mol Genet Metab Rep. 2016; 8:28–32.11. Sage-Schwaede A, Engelstad K, Salazar R, Curcio A, Khandji A, Garvin JH Jr, et al. Exploring mTOR inhibition as treatment for mitochondrial disease. Ann Clin Transl Neurol. 2019; 6:1877–1881.12. Hanaford A, Johnson SC. The immune system as a driver of mitochondrial disease pathogenesis: a review of evidence. Orphanet J Rare Dis. 2022; 17:335.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Leigh Syndrome Mimicking Wernicke's Encephalopathy: A Case Report
- Cardiac Arrest as the Initial Presentation of Leigh Syndrome Associated with Novel NDUFS1 Mutation
- Serial MRI Findings in a Clinically Diagnosed Adult Onset Leigh Syndrome
- Identification of causative mutations in patients with Leigh syndrome and MERRF by mitochondrial DNA-targeted next-generation sequencing
- Arterial hypertension in Leigh syndrome due to m.13513G > A is multicausal, requiring an extensive search to identify its pathphysiology
