Diffuse large B-cell lymphoma presenting as transverse myelitis
- Zukhriddin U
 1
1 - Kang JJ2,3
- Jeong MJ3,4
- Oh SY2,3
- Affiliations
-
- 1Department of Medicine, School of Medicine, Jeonbuk National University, Jeonju, Korea
- 2Department of Neurology, Jeonbuk National University Hospital, Jeonbuk National University School of Medicine, Jeonju, Korea
- 3Research Institute of Clinical Medicine of Jeonbuk National University-Jeonbuk National University Hospital, Jeonju, Korea
- 4Department of Pathology, Jeonbuk National University School of Medicine, Jeonju, Korea
- KMID: 2535723
- DOI: http://doi.org/10.14253/acn.2022.24.2.79
Abstract
- Diffuse large B-cell lymphoma (DLBCL) is the most common type of non-Hodgkin’s lymphoma. Although progressive lymphadenopathy is a typical feature, extranodal involvement may also occur, including the gastrointestinal tract, skin, bone, thyroid, and testes. Central nervous system invasion is rare, so differentiating it from diseases such as inflammatory demyelinating disorder or infection is essential. DLBCL is therefore a challenge to diagnose, especially when the first findings are neurological symptoms. We report an unusual case of DLBCL that presented as transverse myelitis.
Figure
-
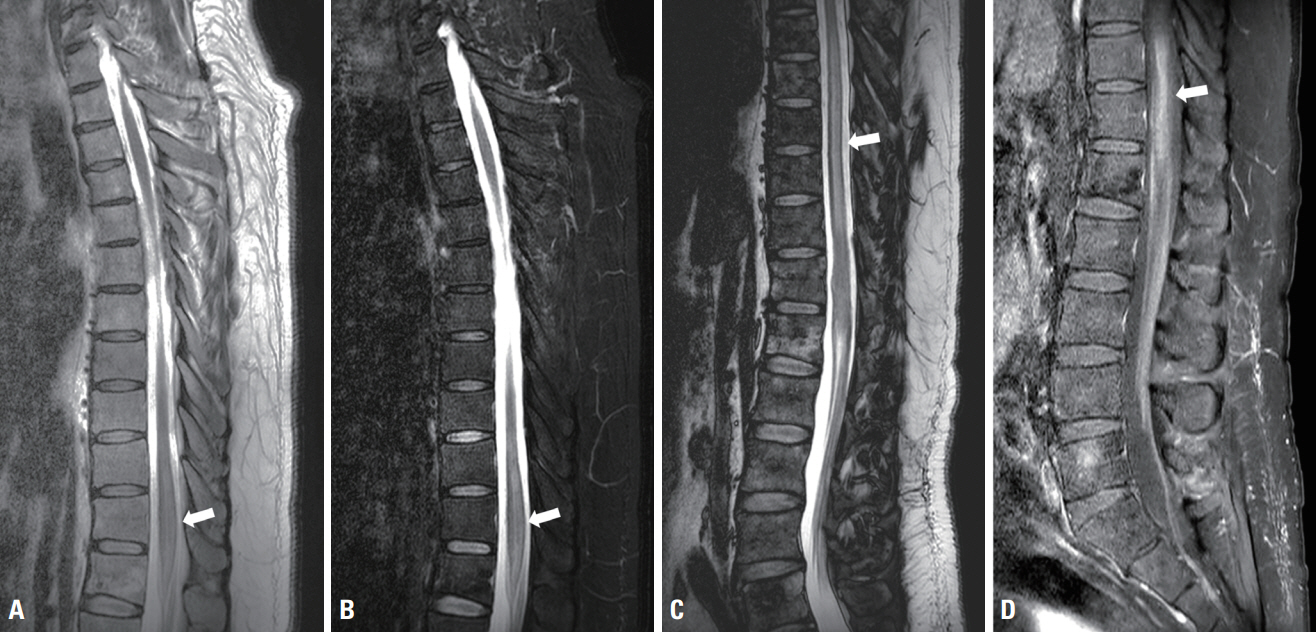
Fig. 1. Magnetic resonance imaging of the spine was performed initially and 15 days after symptom onset. Initial T2-weighted (A) and postcontrast T1-weighted (B) images present mild cord swelling with T2-weighted hyperintensity without enhancement at the T11 and T12 levels (white arrow). Follow-up T2-weighted image (C) and gadolinium-enhanced T1-weighted image (D) demonstrate longitudinally extensive lesions over six vertebral segments (T7 to T12), with accompanying diffuse enhancement (white arrow).
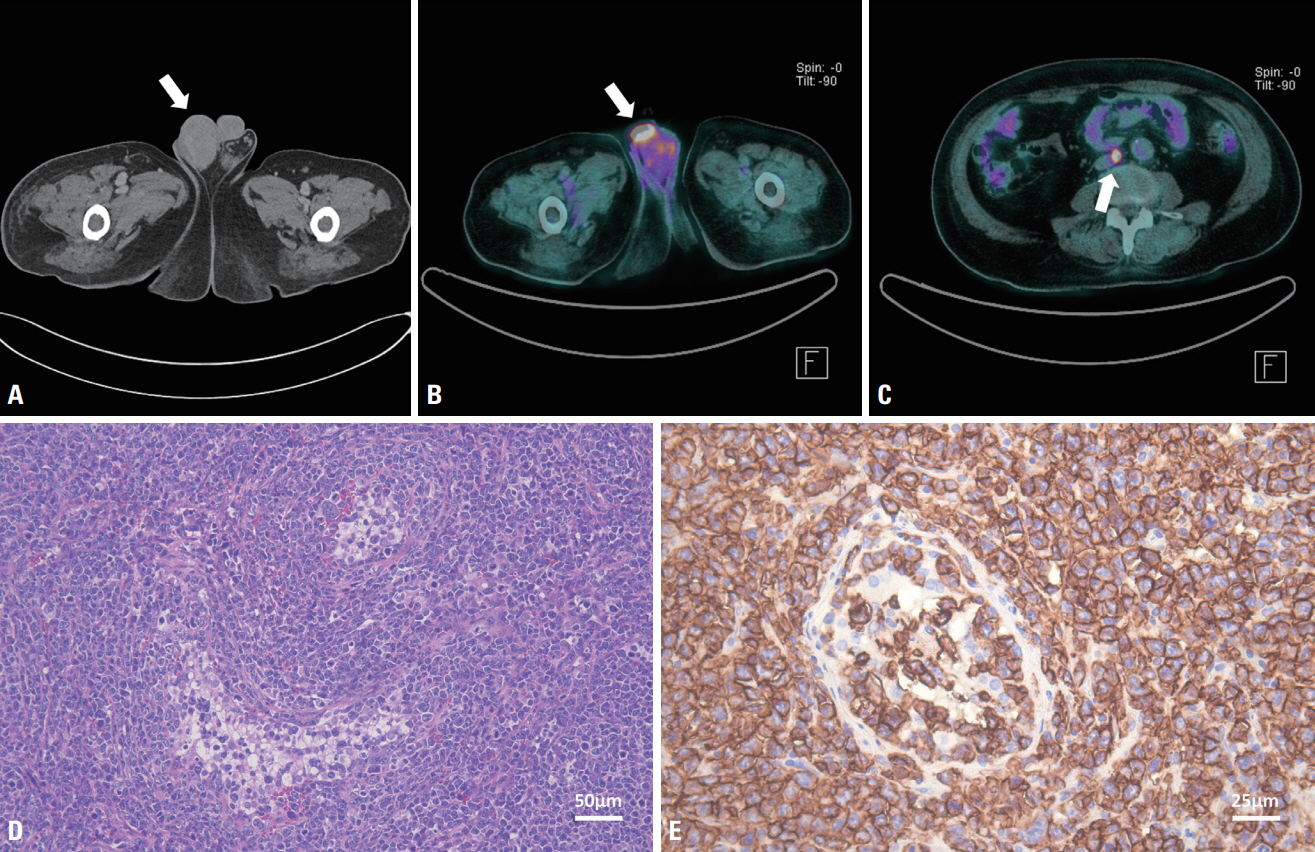
Fig. 2. Computed tomography (CT) of the abdomen and pelvic cavity revealed swelling of the right testis (arrow) with heterogeneous enhancement (A). Fluorodeoxyglucose (FDG) positron-emission tomography/CT performed after right orchiectomy demonstrating mild diffuse hypermetabolism (arrow) thought to be due to a postoperative change in the right inguinal area (B) and an intense FDG-avid small lymph node (arrow) in the aortocaval area (C). The pathological findings demonstrate large atypical lymphocytes replacing the testis (D; Hematoxylin and Eosin staining, ×200) and tumor cells expressing CD20 (a B-cell marker), with the Ki-67 labeling index approaching 90% (E; Immunohistochemical stain, ×400).
Reference
-
1. Sehn LH, Salles G. Diffuse large B-cell lymphoma. N Engl J Med. 2021; 384:842–858.2. Li S, Young KH, Medeiros LJ. Diffuse large B-cell lymphoma. Pathology. 2018; 50:74–87.3. Shi Y, Han Y, Yang J, Liu P, He X, Zhang C, et al. Clinical features and outcomes of diffuse large B-cell lymphoma based on nodal or extranodal primary sites of origin: analysis of 1,085 WHO classified cases in a single institution in China. Chin J Cancer Res. 2019; 31:152–161.4. Chen Y, Lin C, Zhang B. Non-Hodgkin lymphoma with longitudinally extensive transverse myelopathy as the initial symptom: a case report. Front Oncol. 2019; 9:266.5. Kim HS, Kim KK, Kim OJ. A case of diffuse large B-cell lymphoma presenting as transverse myelopathy. J Neurocrit Care. 2008; 1:177–180.6. Kumar N, Keegan BM, Rodriguez FJ, Hammack JE, Kantarci OH. Intravascular lymphoma presenting as a longitudinally-extensive myelitis: diagnostic challenges and etiologic clues. J Neurol Sci. 2011; 303:146–149.7. Ferreri AJ, Campo E, Seymour JF, Willemze R, Ilariucci F, Ambrosetti A, et al. Intravascular lymphoma: clinical presentation, natural history, management and prognostic factors in a series of 38 cases, with special emphasis on the ‘cutaneous variant’. Br J Haematol. 2004; 127:173–183.8. Frohman EM, Wingerchuk DM. Clinical practice. Transverse myelitis. N Engl J Med. 2010; 363:564–572.9. Tolvaj B, Hahn K, Nagy Z, Vadvári Á, Csomor J, Gelpi E, et al. Life threatening rare lymphomas presenting as longitudinally extensive transverse myelitis: a diagnostic challenge. Ideggyogy Sz. 2020; 73:275–285.10. Yunoki M, Suzuki K, Uneda A, Yoshino K. A case of intravascular lymphoma presenting as myelopathy diagnosed with a skin biopsy. Surg Neurol Int. 2015; 6(Suppl 13):S367–S370.11. Merino A. Diffuse large B cell lymphoma presenting as transverse myelitis. Minn Med. 2015; 98:46.12. Shea L, Zhao Y, Reddy V, Yacoubian T, Mehta A. Primary bone marrow diffuse large B-cell lymphoma presenting as transverse myelitis. Am J Med Sci. 2018; 356:561–566.13. Kim H, Nam TS, Levy M, Lee KH, Kim J, Lee SJ. Primary central nervous system lymphoma with intramedullary spinal cord involvement mimicking inflammatory demyelinating disease. J Neurocrit Care. 2019; 12:55–63.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Epstein-Barr Virus-Positive Diffuse Large B-Cell Lymphoma Occurring in Thyroid Gland
- A Case of Acute Transverse Myelitis with Hepatitis B Virus Infection
- Relapse of Ocular Lymphoma following Primary Testicular Diffuse Large B-cell Lymphoma
- Diffuse large B-cell lymphoma presenting with cholecystitis-like symptoms
- A Case of Transverse Myelitis as a First Manifestation of Systemic Lupus Erythematosus
