J Stroke.
2022 Sep;24(3):396-403. 10.5853/jos.2022.00906.
Mechanical Thrombectomy in Acute Stroke Patients with Moderate to Severe Pre-Stroke Disability
- Sykora M
 1,2
1,2 - Michel P3
- Strambo D3
- Krebs S1
- Ferrari J1
- Posekany A4,5
- Mikšová D4
- Hermann K2
- Gattringer T6,7
- Gizewski E8,9
- Deutschmann H7
- Neumann C10
- Lang W1,2
- Affiliations
-
- 1Department of Neurology, St. John’s Hospital, Vienna, Austria
- 2Medical Faculty, Sigmund Freud University Vienna, Vienna, Austria
- 3Stroke Center, Neurology Service, Department of Clinical Neurosciences, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
- 4Austrian National Public Health Institute (Gesundheit Osterreich GmbH)/The Austrian National Institute for Quality in Health Care (Bundesinstitut fur Qualitat im Gesundheitswesen, BIQG), Vienna, Austria
- 5Research Unit of Computational Statistics, University of Technology, Vienna, Austria
- 6Department of Neurology, Medical University of Graz, Graz, Austria
- 7Division of Neuroradiology, Vascular and Interventional Radiology, Department of Radiology, Medical University of Graz, Graz, Austria
- 8Department of Neuroradiology, Medical University of Innsbruck, Innsbruck, Austria
- 9Neuroimaging Research Core Facility, Medical University of Innsbruck, Innsbruck, Austria
- 10Department of Radiology, St. John’s Hospital, Vienna, Austria
- KMID: 2534269
- DOI: http://doi.org/10.5853/jos.2022.00906
Abstract
- Background and Purpose
Studies on mechanical thrombectomy (MT) in acute ischemic stroke (AIS) patients with preexisting disability are limited. We aimed to compare the outcomes of MT versus best medical treatment (BMT) in these patients. Methods In the nationwide Austrian registry and Swiss monocentric registry, we identified 462 AIS patients with pre-stroke disability (modified Rankin Scale [mRS] score ≥3) and acute large vessel occlusion. The primary outcome was returning to pre-stroke mRS or better at 3 months. Secondary outcomes were early neurological improvement (National Institutes of Health Stroke Scale score improvement ≥8 at 24 to 48 hours), 3-month mortality, and symptomatic intracerebral hemorrhage (sICH). Multivariable regression models and propensity score matching (PSM) were used for statistical analyses. Results Compared with the BMT group (n=175), the MT group (n=175) had younger age, more severe strokes, and lower pre-stroke mRS, but similar proportion of receiving intravenous thrombolysis. MT was associated with higher odds of returning to baseline mRS or better at 3 months (adjusted odds ratio [aOR], 2.5; 95% confidence interval [CI], 1.39 to 4.47), early neurological improvement (aOR, 2.62; 95% CI, 1.41 to 4.88), and lower risk of 3-month mortality (aOR, 0.29; 95% CI, 0.18 to 0.49). PSM analysis showed similar findings. MT was not associated with an increased risk of sICH (4.0% vs. 2.1% in all patients; 4.2% vs. 2.4% in the PSM cohort). Conclusions MT in patients with pre-stroke mRS ≥3 might improve the 3-month outcomes and short-term neurological impairment, suggesting that pre-stroke disability alone should not be a reason to withhold MT, but that individual case-by-case decisions may be more appropriate.
Keyword
Figure
-
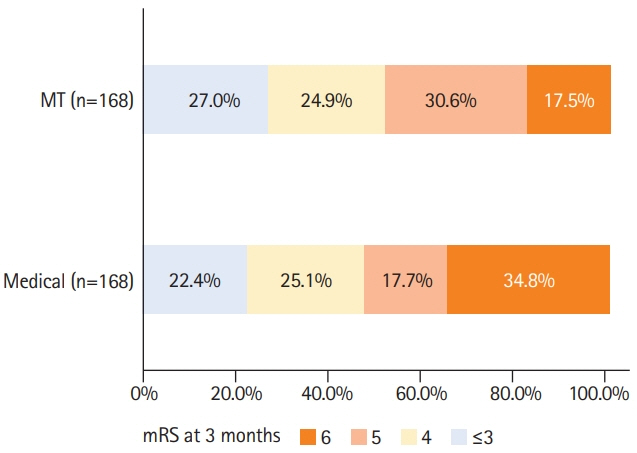
Figure 1. Distribution of modified Ranking Scale (mRS) score at 3 months for mechanical thrombectomy (MT) versus best medical treatment in stroke patients with pre-stroke mRS ≥3 after propensity score matching.
Reference
-
References
1. Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016; 387:1723–1731.2. Albers GW, Marks MP, Kemp S, Christensen S, Tsai JP, Ortega-Gutierrez S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 2018; 378:708–718.3. Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2018; 378:11–21.4. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019; 50:e344–e418.5. Karlinski M, Kobayashi A, Czlonkowska A, Mikulik R, Vaclavik D, Brozman M, et al. Role of preexisting disability in patients treated with intravenous thrombolysis for ischemic stroke. Stroke. 2014; 45:770–775.6. Ganesh A, Luengo-Fernandez R, Pendlebury ST, Rothwell PM. Long-term consequences of worsened poststroke status in patients with premorbid disability. Stroke. 2018; 49:2430–2436.7. Goldhoorn RB, Verhagen M, Dippel DW, van der Lugt A, Lingsma HF, Roos YB, et al. Safety and outcome of endovascular treatment in prestroke-dependent patients. Stroke. 2018; 49:2406–2414.8. Salwi S, Cutting S, Salgado AD, Espaillat K, Fusco MR, Froehler MT, et al. Mechanical thrombectomy in patients with ischemic stroke with prestroke disability. Stroke. 2020; 51:1539–1545.9. de Havenon A, Castonguay A, Nogueira R, Nguyen TN, English J, Satti SR, et al. Prestroke disability and outcome after thrombectomy for emergent anterior circulation large vessel occlusion stroke. Neurology. 2021; 97:e1914–e1919.10. Tanaka K, Yamagami H, Yoshimoto T, Uchida K, Morimoto T, Toyoda K, et al. Endovascular therapy for acute ischemic stroke in patients with prestroke disability. J Am Heart Assoc. 2021; 10:e020783.11. Steiner MM, Brainin M; Austrian Stroke Registry for Acute Stroke Units. The quality of acute stroke units on a nation-wide level: the Austrian Stroke Registry for acute stroke units. Eur J Neurol. 2003; 10:353–360.12. Michel P, Odier C, Rutgers M, Reichhart M, Maeder P, Meuli R, et al. The Acute STroke Registry and Analysis of Lausanne (ASTRAL): design and baseline analysis of an ischemic stroke registry including acute multimodal imaging. Stroke. 2010; 41:2491–2498.13. Bonita R, Beaglehole R. Recovery of motor function after stroke. Stroke. 1988; 19:1497–1500.14. Brott T, Adams HP Jr, Olinger CP, Marler JR, Barsan WG, Biller J, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. 1989; 20:864–870.15. Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008; 359:1317–1329.16. Seker F, Pfaff J, Schönenberger S, Herweh C, Nagel S, Ringleb PA, et al. Clinical outcome after thrombectomy in patients with stroke with premorbid modified Rankin Scale scores of 3 and 4: a cohort study with 136 patients. AJNR Am J Neuroradiol. 2019; 40:283–286.17. Kastrup A, Roth C, Politi M, Alexandrou M, Hildebrandt H, Schröter A, et al. Endovascular therapy vs. thrombolysis in pre-stroke dependent patients with large vessel occlusions within the anterior circulation. Front Neurol. 2021; 12:666596.18. Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet. 2000; 355:1670–1674.19. Young MJ, Regenhardt RW, Sokol LL, Leslie-Mazwi TM. When should neuroendovascular care for patients with acute stroke be palliative? AMA J Ethics. 2021; 23:E783–E793.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Treatment of Acute Ischemic Stroke
- Differences in Effectiveness among Devices for Endovascular Thrombectomy in Patients with Acute Ischemic Stroke
- Intravenous Thrombolysis and Endovascular Thrombectomy in Acute Ischemic Stroke with Minor Symptom
- Recurrent Cardioembolic Stroke Treated Successfully with Repeated Mechanical Thrombectomy within the Acute Index Stroke Period
- Forced Arterial Suction Thrombectomy Using Distal Access Catheter in Acute Ischemic Stroke
