Effect of Estrogen Receptor Expression Level and Hormonal Therapy on Prognosis of Early Breast Cancer
- Affiliations
-
- 1Department of Surgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
- 2Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
- 3Department of Radiology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
- 4Department of Pathology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
- KMID: 2534187
- DOI: http://doi.org/10.4143/crt.2021.890
Abstract
- Purpose
Estrogen receptor (ER) expression in breast cancer plays an essential role in carcinogenesis and disease progression. Recently, tumors with low level (1%-10%) of ER expression have been separately defined as ER low positive (ERlow). It is suggested that ERlow tumors might be morphologically and behaviorally different from tumors with high ER expression (ERhigh).
Materials and Methods
Retrospective analysis of a prospective cohort database was performed. Patients who underwent curative surgery for early breast cancer and had available medical records were included for analysis. Difference in clinicopathological characteristics, endocrine responsiveness and five-year recurrence-free survival was evaluated between different ER subgroups (ERhigh, ERlow, and ER-negative [ER–]).
Results
A total of 2,162 breast cancer patients were included in the analysis, Tis and T1 stage. Among them, 1,654 (76.5%) were ERhigh, 54 (2.5%) were ERlow, and 454 (21.0%) were ER- patients. ERlow cases were associated with smaller size, higher histologic grade, positive human epidermal growth factor receptor 2, negative progesterone receptor, and higher Ki-67 expression. Recurrence rate was highest in ER– tumors and was inversely proportional to ER expression. Recurrence-free survival was not affected by hormonal therapy in the ERlow group (p=0.418).
Conclusion
ERlow breast cancer showed distinct clinicopathological features. ERlow tumors seemed to have higher recurrence rates compared to ERhigh tumors, and they showed no significant benefit from hormonal therapy. Future large scale prospective studies are necessary to validate the treatment options for ERlow breast cancer.
Figure
-

Fig. 1 Survival analysis between different estrogen receptor (ER) subgroups in early breast cancer patients. Difference in 5-year recurrence-free survival between ERhigh/ERlow/ER− (A), ERhigh/ER− (B), ERhigh/ERlow (C), and ERlow/ER− (D) patients. ER−, estrogen receptor negative; ERhigh, estrogen receptor high positive; ERlow, estrogen receptor low positive.
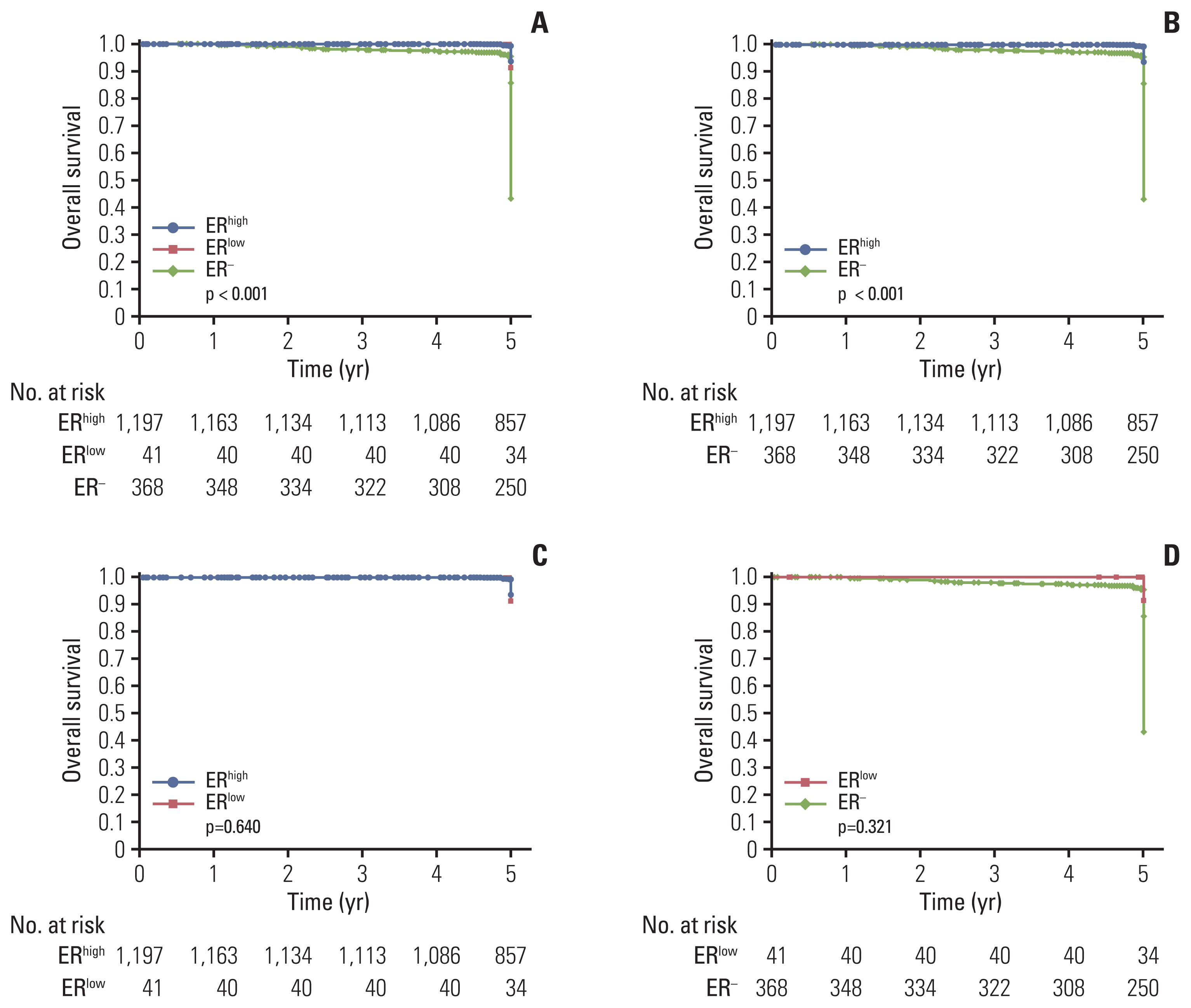
Fig. 2 Survival analysis between different estrogen receptor (ER) subgroups in early stage invasive ductal carcinoma patients. Difference in 5-year recurrence-free survival between ERhigh/ERlow/ER− (A), ERhigh/ER− (B), ERhigh/ERlow (C), and ERlow/ER− (D) patients. ER−, estrogen receptor negative; ERhigh, estrogen receptor high positive; ERlow, estrogen receptor low positive.
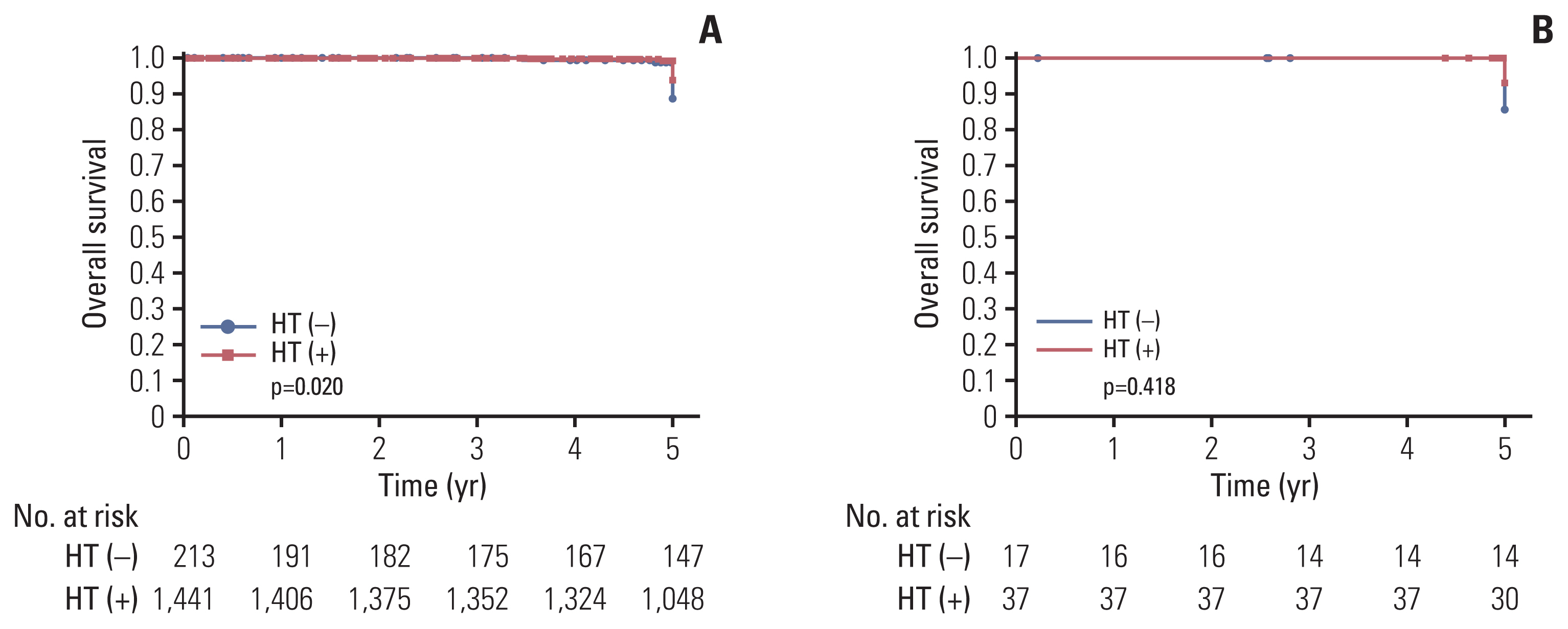
Fig. 3 Effect of estrogen receptor (ER) expression level on hormonal therapy (HT) response. (A) Difference in 5-year recurrence-free survival in ERhigh patients. (B) Difference in 5-year recurrence-free survival in ERlow patients. ERhigh, estrogen receptor high positive; ERlow, estrogen receptor low positive.
Reference
-
References
1. Polyak K. Heterogeneity in breast cancer. J Clin Invest. 2011; 121:3786–8.2. Sestak I. Risk stratification in early breast cancer in premenopausal and postmenopausal women: integrating genomic assays with clinicopathological features. Curr Opin Oncol. 2019; 31:29–34.3. Yip CH, Rhodes A. Estrogen and progesterone receptors in breast cancer. Future Oncol. 2014; 10:2293–301.4. Balleine RL, Wilcken NR. High-risk estrogen-receptor-positive breast cancer: identification and implications for therapy. Mol Diagn Ther. 2012; 16:235–40.5. Anderson WF, Chatterjee N, Ershler WB, Brawley OW. Estrogen receptor breast cancer phenotypes in the Surveillance, Epidemiology, and End Results database. Breast Cancer Res Treat. 2002; 76:27–36.6. Althuis MD, Fergenbaum JH, Garcia-Closas M, Brinton LA, Madigan MP, Sherman ME. Etiology of hormone receptor-defined breast cancer: a systematic review of the literature. Cancer Epidemiol Biomarkers Prev. 2004; 13:1558–68.7. Early Breast Cancer Trialists’ Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005; 365:1687–717.8. Davies E, Hiscox S. New therapeutic approaches in breast cancer. Maturitas. 2011; 68:121–8.9. Allison KH, Hammond ME, Dowsett M, McKernin SE, Carey LA, Fitzgibbons PL, et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP Guideline Update. J Clin Oncol. 2020; 38:1346–66.10. Honma N, Horii R, Iwase T, Saji S, Younes M, Ito Y, et al. Proportion of estrogen or progesterone receptor expressing cells in breast cancers and response to endocrine therapy. Breast. 2014; 23:754–62.11. Balduzzi A, Bagnardi V, Rotmensz N, Dellapasqua S, Montagna E, Cardillo A, et al. Survival outcomes in breast cancer patients with low estrogen/progesterone receptor expression. Clin Breast Cancer. 2014; 14:258–64.12. Gloyeske NC, Dabbs DJ, Bhargava R. Low ER+ breast cancer: is this a distinct group? Am J Clin Pathol. 2014; 141:697–701.13. Heldring N, Pike A, Andersson S, Matthews J, Cheng G, Hartman J, et al. Estrogen receptors: how do they signal and what are their targets. Physiol Rev. 2007; 87:905–31.14. Van den Eynden GG, Colpaert CG, Vermeulen PB, Weyler JJ, Goovaerts G, van Dam P, et al. Comparative analysis of the biochemical and immunohistochemical determination of hormone receptors in invasive breast carcinoma influence of the tumor-stroma ratio. Pathol Res Pract. 2002; 198:517–24.15. Sparano JA, Paik S. Development of the 21-gene assay and its application in clinical practice and clinical trials. J Clin Oncol. 2008; 26:721–8.16. Andre F, Broglio K, Roche H, Martin M, Mackey JR, Penault-Llorca F, et al. Estrogen receptor expression and efficacy of docetaxel-containing adjuvant chemotherapy in patients with node-positive breast cancer: results from a pooled analysis. J Clin Oncol. 2008; 26:2636–43.17. Chen T, Zhang N, Moran MS, Su P, Haffty BG, Yang Q. Borderline ER-positive primary breast cancer gains no significant survival benefit from endocrine therapy: a systematic review and meta-analysis. Clin Breast Cancer. 2018; 18:1–8.18. Hammond ME, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, et al. American Society of Clinical Oncology/College Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol. 2010; 28:2784–95.19. Yi M, Huo L, Koenig KB, Mittendorf EA, Meric-Bernstam F, Kuerer HM, et al. Which threshold for ER positivity? a retrospective study based on 9639 patients. Ann Oncol. 2014; 25:1004–11.20. Poon IK, Tsang JY, Li J, Chan SK, Shea KH, Tse GM. The significance of highlighting the oestrogen receptor low category in breast cancer. Br J Cancer. 2020; 123:1223–7.21. Viale G, Regan MM, Maiorano E, Mastropasqua MG, Dell’Orto P, Rasmussen BB, et al. Prognostic and predictive value of centrally reviewed expression of estrogen and progesterone receptors in a randomized trial comparing letrozole and tamoxifen adjuvant therapy for postmenopausal early breast cancer: BIG 1–98. J Clin Oncol. 2007; 25:3846–52.22. Ogawa Y, Moriya T, Kato Y, Oguma M, Ikeda K, Takashima T, et al. Immunohistochemical assessment for estrogen receptor and progesterone receptor status in breast cancer: analysis for a cut-off point as the predictor for endocrine therapy. Breast Cancer. 2004; 11:267–75.23. Collins LC, Botero ML, Schnitt SJ. Bimodal frequency distribution of estrogen receptor immunohistochemical staining results in breast cancer: an analysis of 825 cases. Am J Clin Pathol. 2005; 123:16–20.24. Fujii T, Kogawa T, Dong W, Sahin AA, Moulder S, Litton JK, et al. Revisiting the definition of estrogen receptor positivity in HER2-negative primary breast cancer. Ann Oncol. 2017; 28:2420–8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endocrine Therapy for Breast Cancer
- The Relationship Between the Expression of Estrogen Receptor beta and Recurrence in Breast Cancer
- Expression of the pS2 Protein and Its Relation with Estrogen and Progesterone Receptor in Breast Cancer
- Pattern Alopecia during Hormonal Anticancer Therapy in Patients with Breast Cancer
- Clinical Significance of DAX-1 Expression using Immunihistochemical Staining in Breast Cancer
