Papillary and medullary thyroid carcinomas coexisting in the same lobe, first suspected based on fine-needle aspiration cytology: a case report
- Affiliations
-
- 1Department of Pathology and Translational Genomics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 2Department of Pathology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2533707
- DOI: http://doi.org/10.4132/jptm.2022.08.03
Abstract
- Because different types of thyroid malignancies have distinct embryological origins, coexisting tumors are rarely observed. We describe a coexisting papillary thyroid carcinoma (PTC) and medullary thyroid carcinoma (MTC) first suspected by fine-needle aspiration cytology (FNAC). A 57-year-old female presented with an irregular mass in the right thyroid lobe. The cytopathologic findings of fine-needle aspiration showed two components: a papillary-like arrangement consisting of cells with pale enlarged nuclei indicative of PTC and loose clusters comprised of oval cells with granular chromatin indicative of MTC. The diagnosis of a coexisting PTC and MTC was initially confirmed by calcitonin immunocytochemistry and later after total thyroidectomy. Although some surgical case reports of PTC and MTC coexisting in either the same or different lobes have been documented, a case suspected by FNAC before the surgery has rarely been reported. Because appropriate treatment and prognosis of PTC and MTC are different, cytopathologists should be aware of this rare entity.
Figure
-
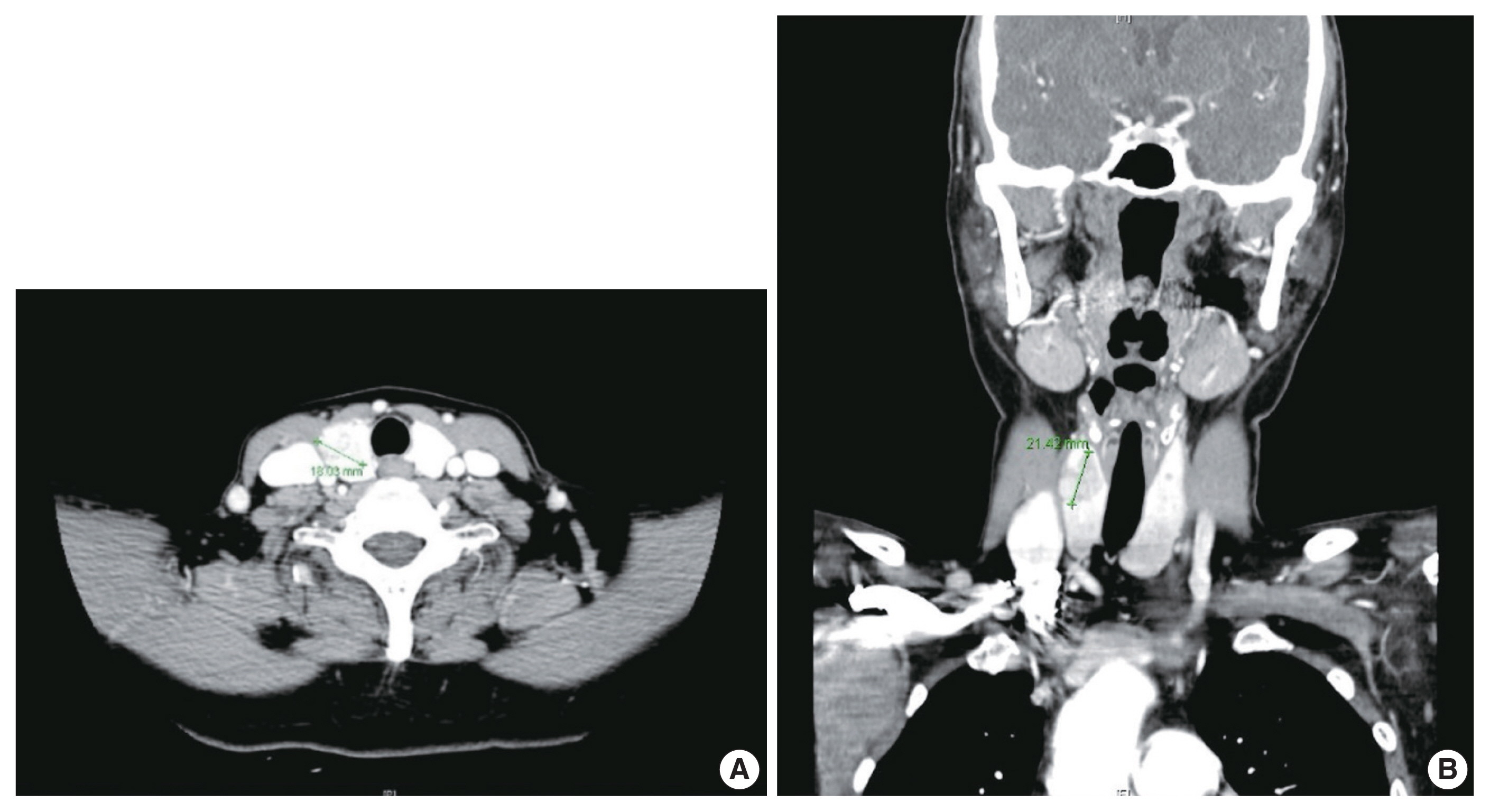
Fig. 1 Initial head and neck computed tomography scan in the cross (A) and transverse (B) view showing a calcified mass-like lesion measuring 2.1 × 1.8 cm in the right thyroid lobe.

Fig. 2 Fine-needle aspiration cytology (FNAC) of the mass in the right thyroid lobe. (A) Low-power view of FNAC demonstrates dispersed single cells and syncytial-type tissue fragments. (B) Loose cellular aggregates show a mixture of oval- to spindle-shaped tumor cells with various chromatin patterns. (C) Two distinct clusters with cytologically different features: syncytium-like arrangement consisting of neoplastic cells with nuclear enlargement, crowding, and chromatin clearing (asterisk) and loose clusters with a streaming pattern composed of oval- to spindle-shaped tumor cells with smooth nuclear membrane (double asterisk). (D) High-power view of cytologic features of papillary carcinoma shows cellular syncytium composed of cells with irregular nuclear membrane, nuclear groove, and nuclear clearing (Papanicolaou stain). (E) The presence of concentric lamellated calcified structures (arrowheads), known as psammoma bodies, is a diagnostic histologic feature of papillary carcinoma. The presence of intranuclear pseudo-inclusion (black circle) supports the presence of the papillary carcinoma component but can also be observed in the medullary carcinoma component (Papanicolaou stain). (F) Some multinucleated giant cells (arrowheads) are also observed in the papillary carcinoma (Papanicolaou stain). (G) High-power view of cytologic features of medullary carcinoma shows oval- to spindle-shaped dispersed cells with granular chromatin. (H) The component suspicious for medullary carcinoma shows diffuse and strong cytoplasmic and nuclear positivity in the immunocytochemical staining for calcitonin.

Fig. 3 Gross and microscopic presentation of the right thyroid lobe of total thyroidectomy specimen. (A) A well-demarcated multinodular yellowish mass measuring 1.9 × 1.8 cm in the upper-to-mid portion. After microscopic evaluation, a well-demarcated yellowish nodular lesion (double asterisk) is determined to be a medullary carcinoma component and the other infiltrative irregular lesion (asterisk) a papillary carcinoma component. (B) On the low-power view of the mass including both components, a medullary carcinoma component (double asterisk) is identified immediately adjacent to the papillary carcinoma component (asterisk). The two components are clearly separated from each other by fibrous tissue and intervening normal thyroid tissue. (C, D) Papillary carcinoma component. (C) At low power, an infiltrative border and predominantly papillary complex branching structures are identified. (D) At high power, well-developed papillary architectures lined by cuboidal tumor cells with chromatin clearing are observed. (E, F) Medullary carcinoma component. (E) At low power, a lobulated cellular mass composed of several nests of neoplastic cells is observed. (F) At high power, the tumor consists of multiple nests composed of oval- to spindle-shaped cells with hyperchromatic nuclei. (G, H) Immunohistochemical stain for calcitonin in the histologic specimen. (G) At low power, the papillary carcinoma component (asterisk) shows negativity, and the medullary carcinoma component (double asterisk) shows diffuse and strong positivity for calcitonin. (H) At high power, diffuse and strong positivity, both cytoplasmic and nuclear, in the medullary carcinoma component is observed.
Reference
-
References
1. Kazaure HS, Roman SA, Sosa JA. Aggressive variants of papillary thyroid cancer: incidence, characteristics and predictors of survival among 43,738 patients. Ann Surg Oncol. 2012; 19:1874–80.
Article2. Sadat Alavi M, Azarpira N. Medullary and papillary carcinoma of the thyroid gland occurring as a collision tumor with lymph node metastasis: a case report. J Med Case Rep. 2011; 5:590.
Article3. De Felice M, Di Lauro R. Thyroid development and its disorders: genetics and molecular mechanisms. Endocr Rev. 2004; 25:722–46.
Article4. Baloch ZW, LiVolsi VA. Special types of thyroid carcinoma. Histopathology. 2018; 72:40–52.
Article5. Kimura ET, Nikiforova MN, Zhu Z, Knauf JA, Nikiforov YE, Fagin JA. High prevalence of BRAF mutations in thyroid cancer: genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer Res. 2003; 63:1454–7.6. Marsh DJ, Learoyd DL, Andrew SD, et al. Somatic mutations in the RET proto-oncogene in sporadic medullary thyroid carcinoma. Clin Endocrinol (Oxf). 1996; 44:249–57.7. Alberti L, Carniti C, Miranda C, Roccato E, Pierotti MA. RET and NTRK1 proto-oncogenes in human diseases. J Cell Physiol. 2003; 195:168–86.
Article8. Greco C, Brigante G, Taliani E, Corrado S, Simoni M, Madeo B. Concomitant medullary thyroid carcinoma with paraganglioma-like pattern and papillary thyroid carcinoma. Endocrinol Diabetes Metab Case Rep. 2019; 2019:19–0094.
Article9. Kim WG, Gong G, Kim EY, et al. Concurrent occurrence of medullary thyroid carcinoma and papillary thyroid carcinoma in the same thyroid should be considered as coincidental. Clin Endocrinol (Oxf). 2010; 72:256–63.
Article10. Maitra A. The endocrine system. Kumar V, Abbas AK, Aster JC, editors. Robbins and Cotran pathologic basis of disease. 9th ed. Philadelphia: Elsevier publications;2015. p. 1073–140.
Article11. Braverman LE. Werner and Ingbar’s the thyroid: a fundamental and clinical text. Philadelphia: Lippincott Williams and Wilkins;2005.12. Wells SA Jr, Asa SL, Dralle H, et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid. 2015; 25:567–610.
Article13. Jimenez C, Hu MI, Gagel RF. Management of medullary thyroid carcinoma. Endocrinol Metab Clin North Am. 2008; 37:481–96.
Article14. Rossi S, Fugazzola L, De Pasquale L, et al. Medullary and papillary carcinoma of the thyroid gland occurring as a collision tumour: report of three cases with molecular analysis and review of the literature. Endocr Relat Cancer. 2005; 12:281–9.
Article15. Sizemore GW. Medullary carcinoma of the thyroid gland. Semin Oncol. 1987; 14:306–14.16. Lloyd RV, Osamura RY, Kloppel G, Rosai J. WHO classification of tumours of endocrine organs . 4th ed. Lyon: IARC Press;2017.17. Lamberg BA, Reissel P, Stenman S, et al. Concurrent medullary and papillary thyroid carcinoma in the same thyroid lobe and in siblings. Acta Med Scand. 1981; 209:421–4.
Article18. Younes N, Shomaf M, Al Hassan L. Simultaneous medullary and papillary thyroid carcinoma with lymph node metastasis in the same patient: case report and review of the literature. Asian J Surg. 2005; 28:223–6.
Article19. Ahn D, Sohn JH, Park JY. A case of concurrent papillary and medullary thyroid carcinomas detected as recurrent medullary carcinoma after initial surgery for papillary carcinoma. J Korean Thyroid Assoc. 2013; 6:80–4.
Article20. Ali SZ, Cibas ES. The Bethesda System for Reporting Thyroid Cytopathology: definitions, criteria and explanatory notes. 2nd ed. Cham: Springer;2010.21. Tuttle M, Morris LF, Haugen B, et al. Thyroid-differentiated and anaplastic carcinoma. Amin MB, Edge SB, Greene F, editors. AJCC cancer staging manual. 8th ed. New York: Springer International Publishing;2017. p. 881–98.22. Cibas ES, Ali SZ. The 2017 Bethesda System for Reporting Thyroid Cytopathology. J Am Soc Cytopathol. 2017; 6:217–22.
Article23. Green I, Ali SZ, Allen EA, Zakowski MF. A spectrum of cytomorphologic variations in medullary thyroid carcinoma: fine-needle aspiration findings in 19 cases. Cancer. 1997; 81:40–4.
Article24. Trimboli P, Treglia G, Guidobaldi L, et al. Detection rate of FNA cytology in medullary thyroid carcinoma: a meta-analysis. Clin Endocrinol (Oxf). 2015; 82:280–5.
Article25. Liu CY, Chen CC, Bychkov A, et al. Constitutive cytomorphologic features of medullary thyroid carcinoma using different staining methods. Diagnostics (Basel). 2021; 11:1396.
Article26. Papaparaskeva K, Nagel H, Droese M. Cytologic diagnosis of medullary carcinoma of the thyroid gland. Diagn Cytopathol. 2000; 22:351–8.
Article27. Biscolla RP, Ugolini C, Sculli M, et al. Medullary and papillary tumors are frequently associated in the same thyroid gland without evidence of reciprocal influence in their biologic behavior. Thyroid. 2004; 14:946–52.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Mixed Follicular-Papillary Thyroid Carcinoma
- A Case of Concurrent Medullary and Papillary Carcinoma of the Thyroid Gland
- Concurrent Papillary and Medullary Carcinoma of the Thyroid Gland
- Fine needle aspiration cytology of medullary carcinoma of the thyroid gland: a case report
- A Case of Concurrent Papillary and Medullary Thyroid Carcinomas Detected as Recurrent Medullary Carcinoma after Initial Surgery for Papillary Carcinoma
