A technical note on anterolateral mobilization in vertebrobasilar dolichoectasia for relief of brainstem compression
- Affiliations
-
- 1Department of Neurological Surgery, Oregon Health & Science University, Portland, Oregon, USA
- KMID: 2533683
- DOI: http://doi.org/10.7461/jcen.2022.E2020.11.004
Abstract
- Vascular compression of neural tissue causing neurological symptoms is a wellknown phenomenon. This is commonly seen in trigeminal neuralgia and, less commonly, in hemifacial spasm by small arteries, which can be treated by microvascular decompression. Rarely, larger arteries, such as the vertebral arteries, may compress the brainstem. This can lead to symptoms of pontine or medullary distress like hemiparesis, dysphagia, or respiratory distress. This is treated by macrovascular decompression. Due to the rare and heterogenous nature of this disease, there is no standardized approach. We describe a novel technique whereby the vertebrobasilar system is mobilized anterolaterally towards the occipital condyle with a sling to decompress the brainstem.
We report two cases of vertebrobasilar dolichoectasia causing brainstem compression. A carotid patch graft sling with anterolateral mobilization to the occipital condyle is described as a surgical nuance to macrovascular decompressive surgery. Briefly, the vertebral artery was identified and dissected away from the brainstem and the bulbar cranial nerves. Bovine pericardium graft was used to create a sling around the artery by suturing the two ends together. The sling was then fixed either to the occipital condyle using cranial plating screws or suturing to the dura of the occipital condyle.
A novel surgical technique for management of vertebrobasilar dolichoectasia causing brainstem compression with progressive neurological deterioration is reported. Anatomical location and the offending vessel should guide neurosurgeons to select the best surgical option to achieve complete decompression of the involved neural structures.
Keyword
Figure
-
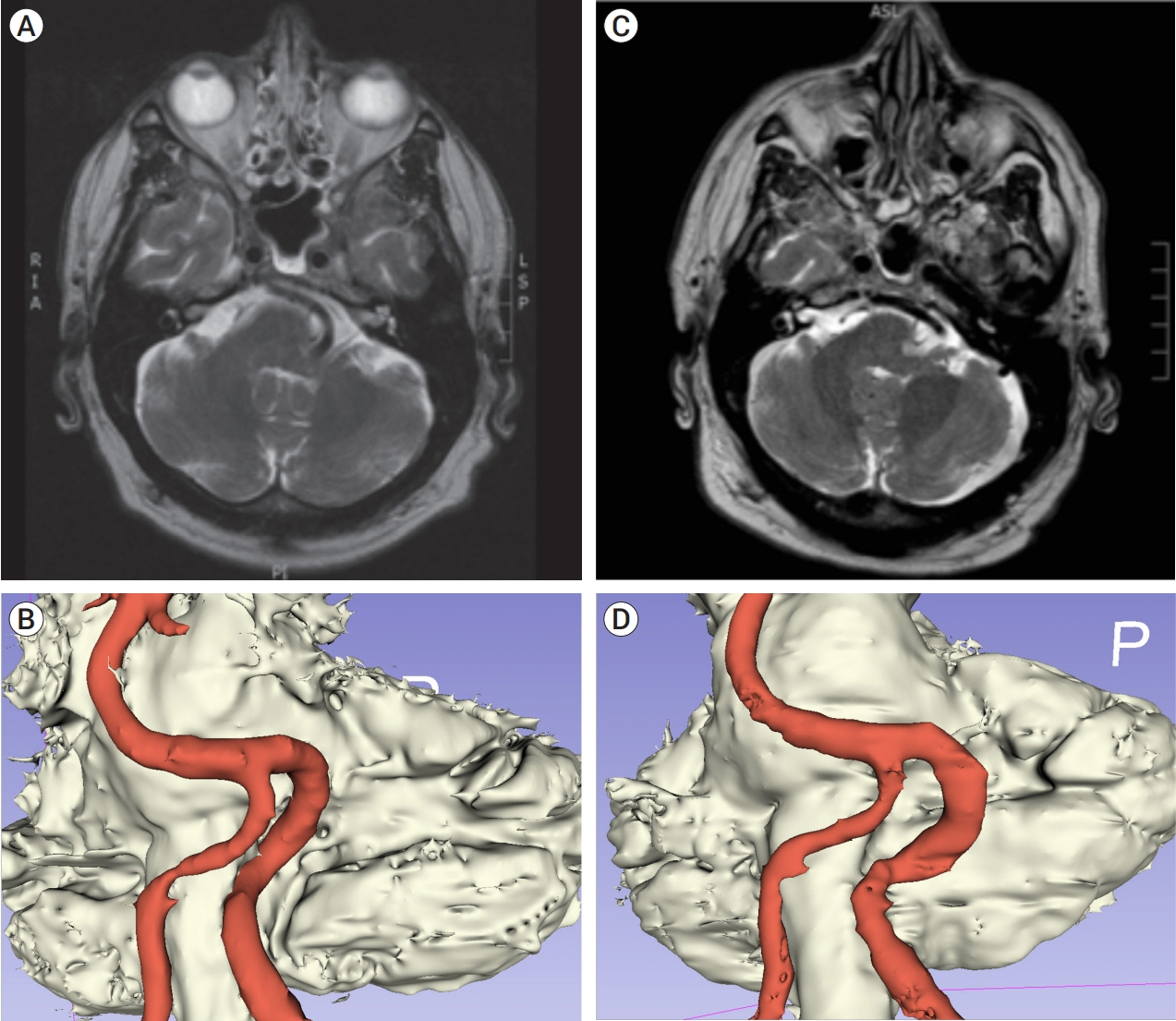
Fig. 1. (A) Pre-operatively obtained axial, T2-weighted MRI image showing significant left brainstem compression by the left vertebral artery. (B) 3D reconstruction of the pre-operative MRI demonstrating severe pontomedullary compression with indentation. (C) Post-operative axial, T2-weighted MRI with decompression of the brainstem with the left vertebral artery iatrogenically displaced anterolaterally. (D) 3D reconstruction of the post-operative MRI demonstrating decompression with residual pontomedullary indentation. MRI, magnetic resonance imaging
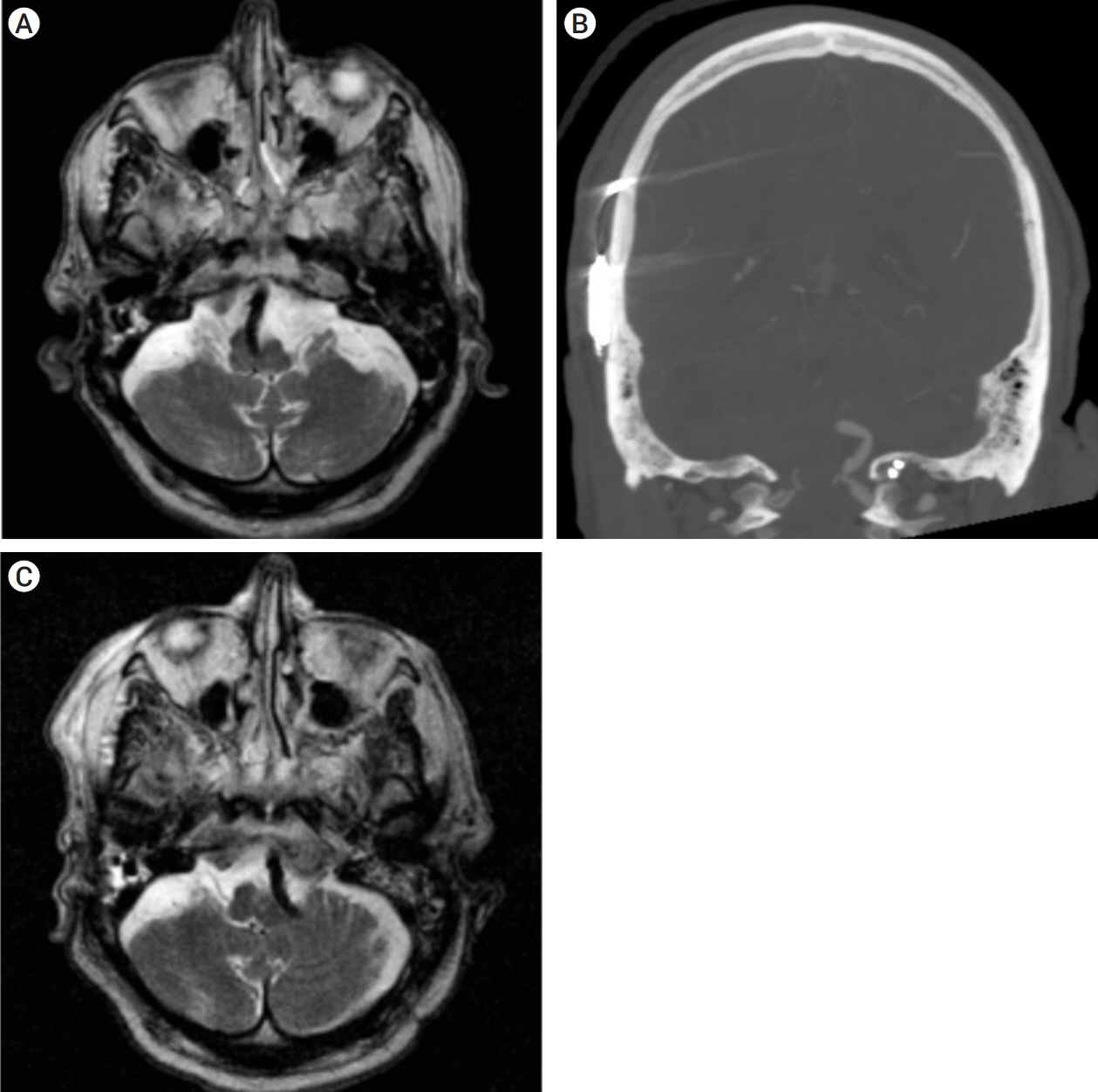
Fig. 2. (A) Pre-operative obtained axial, T2-weighted MRI showing significant medullary compression from the left vertebral artery. (B) Post-operative coronal computed tomography angiography (CTA) showing placement of cranial fixation screws into the occipital condyle with adjacent displaced vertebrobasilar system. (C) Post-operative axial, T2-weighted MRI with substantial decompression of the brainstem with the left vertebral artery iatrogenically displaced anterolaterally. MRI, magnetic resonance imaging

Fig. 3. (A) Intra-operative image demonstrating the medulla (M) with the vertebral artery (VA) being mobilized by closed forceps prior to (B) Intra-operative image showing the VA being wrapped in the Hemashield sling (HS). (C) Intra-operative image of the loose ends of the sling being stitched together by a single suture. (D) Intra-operative picture of the sling mobilizing the VA away from the medulla after anchoring to the dura of the occipital condyle.
Reference
-
1. Baldauf J, Rosenstengel C, Schroeder HWS. Nerve compression syndromes in the posterior cranial fossa. Dtsch Arztebl Int. 2019; Jan. 116(4):54–60.
Article2. Choudhri O, Connolly ID, Lawton MT. Macrovascular decompression of the brainstem and cranial nerves: evolution of an anteromedial vertebrobasilar artery transposition technique. Neurosurgery. 2017; Aug. 81(2):367–76.
Article3. Elias WJ, Burchiel KJ. Microvascular decompression. Clin J Pain. 2002; Jan-Feb. 18(1):35–41.
Article4. Lin CF, Chen HH, Hernesniemi J, Lee CC, Liao CH, Chen SC, et al. An easy adjustable method of ectatic vertebrobasilar artery transposition for microvascular decompression. Clin Neurol Neurosurg. 2012; Sep. 114(7):951–6.
Article5. Munich SA, Morcos JJ. “Macrovascular” decompression of dolichoectatic vertebral artery causing hemifacial spasm using goretex sling: 2-dimensional operative video. Oper Neurosurg (Hagerstown). 2019; Feb. 16(2):267–8.
Article6. Nakahara Y, Kawashima M, Matsushima T, Kouguchi M, Takase Y, Nanri Y, et al. Microvascular decompression surgery for vertebral artery compression of the medulla oblongata: 3 cases with respiratory failure and/or dysphagia. World Neurosurg. 2014; Sep-Oct. 82(3-4):535.e11–6.
Article7. Passero SG, Rossi S. Natural history of vertebrobasilar dolichoectasia. Neurology. 2008; Jan. 70(1):66–72.
Article8. Pico F, Labreuche J, Amarenco P. Pathophysiology, presentation, prognosis, and management of intracranial arterial dolichoectasia. Lancet Neurol. 2015; Aug. 14(8):833–45.
Article9. Raabe A, Jaiimsin A, Seifert V, Beck J. Use of a strip-clip technique to maintain transposition of a vertebral artery in microvascular decompression surgery. Acta Neurochir (Wien). 2011; Dec. 153(12):2393–5.
Article10. Srinivasan VM, Labib MA, Furey CG, Catapano JS, Lawton MT. The “binder ring” bypass: transection, rerouting, and reanastomosis as an alternative to macrovascular decompression of a dolichoectatic vertebral artery. Oper Neurosurg (Hagerstown). 2022; Apr. 22(4):224–30.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of vertebrobasilar dolichoectasia manifesting as sudden sensorineural hearing loss with vertigo
- Huge Vertebrobasilar Dolichoectasia
- Dolichoectasia of vertebrobasilar artery presenting as facial pain: a case report
- Lower Cranial Nerve Palsy Due to Vertebrobasilar Dolichoectasia
- Vestibular Function Test in Old Age Patients with Vertebrobasilar Dolichoectasia
