A Rare Case of Oligodendroglioma in Sacrococcygeal Mature Teratoma Diagnosed in Preterm Infant
- Affiliations
-
- 1Department of Pediatrics, Pusan National University Children’s Hospital, Yangsan, Korea
- 2Department of Pediatrics, Pusan National University School of Medicine, Yangsan, Korea
- 3Department of Pathology, Pusan National University School of Medicine, Yangsan, Korea
- 4Division of Pediatric Surgery, Department of Surgery, Pusan National University Children’s Hospital, Yangsan, Korea
- 5Department of Surgery, Pusan National University School of Medicine, Yangsan, Korea
- KMID: 2533092
- DOI: http://doi.org/10.5385/nm.2022.29.3.105
Abstract
- Sacrococcygeal teratoma is the most common congenital tumor in neonates, and is reported in approximately 1/35,000 to 1/40,000 live births. Oligodendroglioma is a rare central nervous system tumor that is usually found in the cerebral hemisphere of young and middle aged adults. When associated with a teratoma, it is mainly identified in ovarian teratoma in adolescents and adults. We describe a rare case of a preterm infant with oligodendroglioma in a mature sacrococcygeal teratoma. The male neonate was born at a gestational age of 30 weeks with a protruding mass in the sacrococcygeal region. Pelvic magnetic resonance imaging showed a sacrococcygeal teratoma of approximately 11 cm comprising fat components and skeletal structure, that extended from the anterior part of the sacrum to the abdominal cavity. Radical resection was performed at 36 days of age. Macroscopically, the resected intra-abdominal mass had the characteristics of a cystic lesion, and the intrapelvic mass was a predominantly solid mixed cystic-solid lesion. Histologically, this solid lesion in the intrapelvic mass was composed of mature glial tissue, which comprised as a proliferation of monotonous cells with small and round nuclei, surrounded by a perinuclear halo (“fried egg” appearance). Additionally, these cells were immunohistochemically positive for glial fibrillary acidic protein. These findings confirmed the diagnosis of oligodendroglioma in sacrococcygeal mature teratoma. After the treatment, no recurrence was observed during the follow-up period, and no additional intervention was required. However, the patient is undergoing treatment for voiding dysfunction caused by a neurogenic bladder.
Figure
-
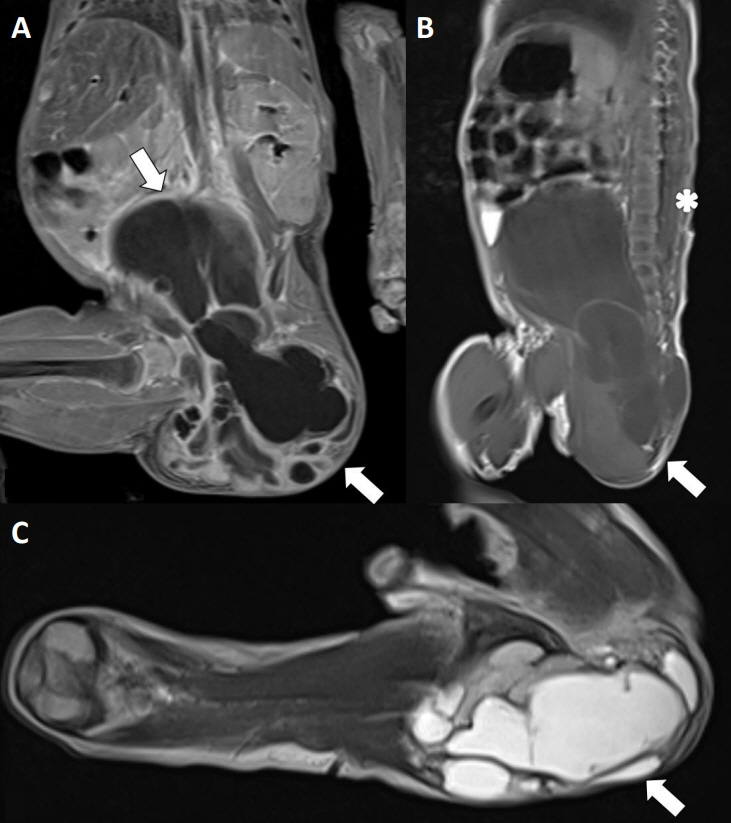
Figure 1. (A) Contrast-enhanced fat-saturated T1-weighted magnetic resonance image (MRI), coronal view (arrows), (B) T1-weighted MRI, sagittal view (arrow), and (C) double fat suppression of T2-weighted MRI, transverse view (arrow) reveals—a multicystic mass with a bony structure and fatty component. The longitudinal dimension of the cystic mass in the coronal image is 11 cm, which extends to the abdomen through the presacral space. The tip of the conus medullaris ends at approximately the L2 vertebra (asterisk).
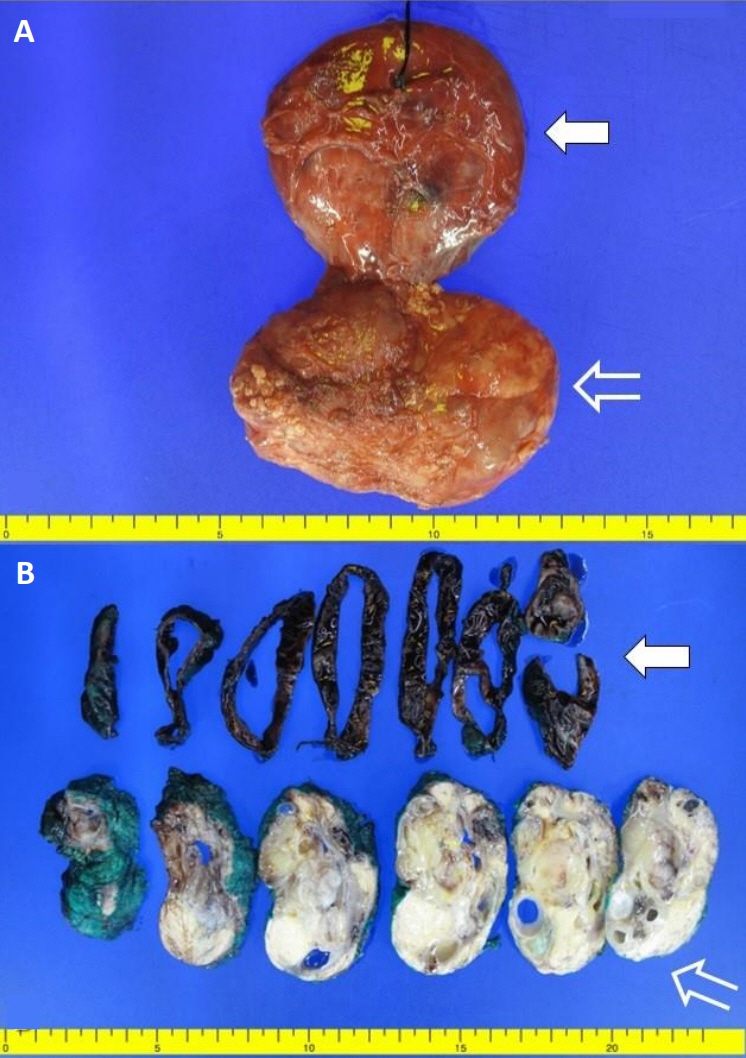
Figure 2. Macroscopic examination shows (A) a mass measuring 12.0×8.1×2.5 cm in size. (B) The mass in the abdominal cavity (arrows) has characteristics of a cystic lesion, and the mass in the pelvis is identified as a mixed cystic-solid mass which is predominantly solid (open arrows).
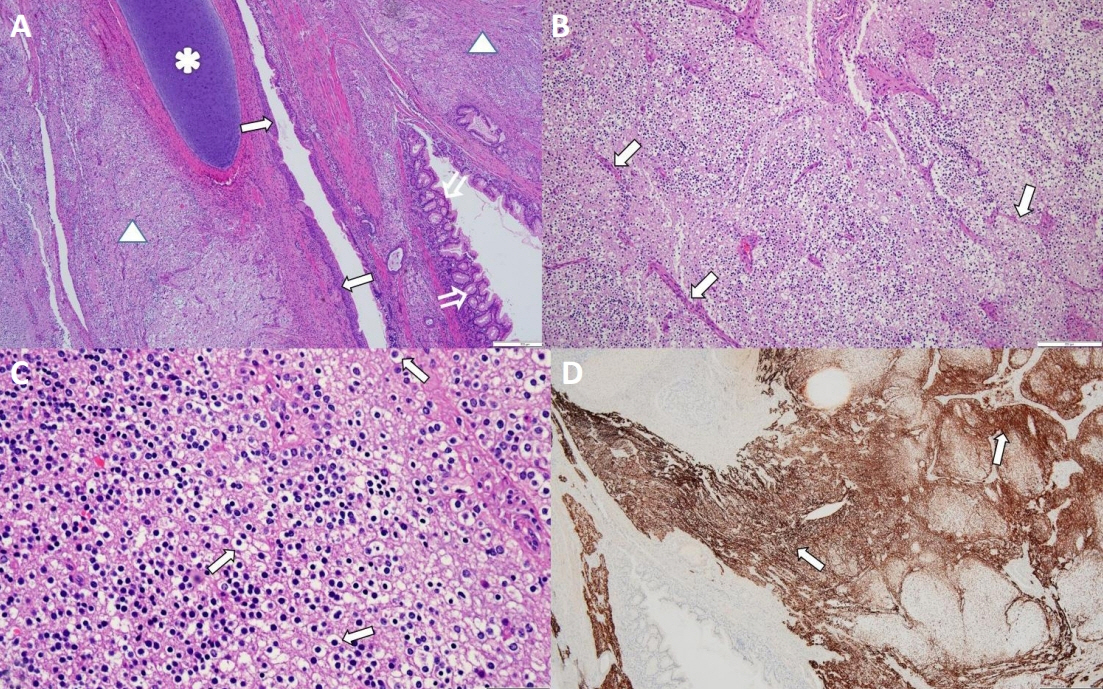
Figure 3. (A) The tumor shows mature cartilages (asterisk), colonic epithelium (open arrows), non-keratinizing squamous epithelium (arrows), and glial tissue (triangles) (hematoxylin and eosin [H&E], ×40). (B) Glial tissue shows uniform round nuclei with clear perinuclear halos, and delicate branching patterns of their vasculature exhibit a “chicken wire” arrangement (arrows) (H&E, ×100). (C) Glial tissue shows proliferation of monotonous cells with small and round nuclei with perinuclear clearing (fried egg appearance) (arrows) (H&E, ×400). (D) Glial tissue is positive for the anti-Glial fibrillary acidic protein antibody (immunoperoxidase staining, ×40) (arrows) (Scale bar, 500 μm).
Reference
-
1. Opris I, Ducrotoy V, Bossut J, Lamy A, Sabourin JC. Oligodendroglioma arising in an ovarian mature cystic teratoma. Int J Gynecol Pathol. 2009; 28:367–71.2. Unal B, Gulec F, Sedele M. Oligodendroglioma arising in mature cystic teratoma. Case Rep Oncol Med. 2014; 2014:745462.3. Tuladhar R, Patole SK, Whitehall JS. Sacrococcygeal teratoma in the perinatal period. Postgrad Med J. 2000; 76:754–9.4. Varras M, Diakakis G, Monselas I, Akrivis C. Prenatal diagnosis of a huge foetal immature sacrococcygeal teratoma: our experience of a rare case and review of the literature. OA Case Rep. 2013; 2:10.5. Jung CK, Lee YS, Jung ES, Kang CS, Kim BK. Oligodendroglioma arising in a sacrococcygeal immature teratoma. J Korean Med Sci. 2002; 17:426–8.6. Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, FigarellaBranger D, et al. The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol. 2021; 23:1231–51.7. Hu Q, Yan Y, Liao H, Liu H, Yu H, Zhao F. Sacrococcygeal teratoma in one twin: a case report and literature review. BMC Pregnancy Childbirth. 2020; 20:751.8. Buyukka Bay S, Corapcioglu F, Kavurt S, Muezzinoglu B, Anik Y, Tugay M. Oligodendroglioma arising in a mature cystic ovarian teratoma in a child. Pediatr Hematol Oncol. 2010; 27:636–40.9. Ud Din N, Memon A, Aftab K, Ahmad Z, Ahmed R, Hassan S. Oligodendroglioma arising in the glial component of ovarian teratomas: a series of six cases and review of literature. J Clin Pathol. 2012; 65:631–4.10. Serrano-Arevalo ML, Lino-Silva LS, Dominguez Malagon HR. Oligodendroglial cell proliferation arising in an ovarian mature cystic teratoma: clinicopathological, inmunohistochemical, and ultrastructural study of a case that may represent an oligodendroglioma. Ultrastruct Pathol. 2017; 41:62–6.11. Hirschowitz L, Ansari A, Cahill DJ, Bamford DS, Love S. Central neurocytoma arising within a mature cystic teratoma of the ovary. Int J Gynecol Pathol. 1997; 16:176–9.12. Zannoni GF, Fadda G, Scambia G, Capelli A, Carbone A. Oligodendroglioma arising within a mature cystic ovarian teratoma: case report and review of the literature. Acta Obstet Gynecol Scand. 2002; 81:896–7.13. Caltabiano R, Lanzafame S. Oligodendroglioma arising in an immature ovarian teratoma: case report. Pathologica. 2008; 100:420–3.14. Panesar NK, Sidhu JS. Uterine cervical teratoma with divergent neuroepithelial differentiation and development of an oligo dendroglioma: report of a case and review of the literature. Ann Diagn Pathol. 2007; 11:293–6.15. Galili O, Mogilner J. Type IV sacrococcygeal teratoma causing urinary retention: a rare presentation. J Pediatr Surg. 2005; 40:E18–20.
