Successful Management of Recurrent Type A Aortic Dissection With Customized Fenestrated Stentgraft in a Patient With High Surgical Risk
- Affiliations
-
- 1Incheon Sejong Hospital, Incheon, Korea
- 2S&G Biotech Incorporated, Seoul, Korea
- 3Cardiovascular Center, Korea University Guro Hospital, Seoul, Korea
- KMID: 2532335
- DOI: http://doi.org/10.4070/kcj.2022.0074
Figure
-
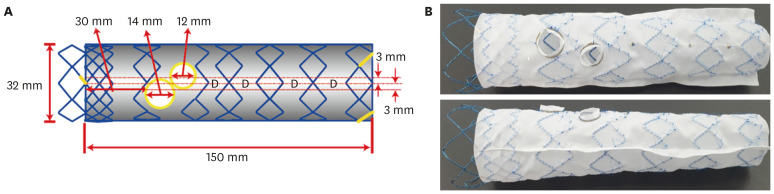
Figure 1 Design and real customized stent graft. (A) Schematic design according to 3D CT and invasive angiography. (B) Real stent-graft product model production.3D = 3-dimensional; CT = computerized tomography.
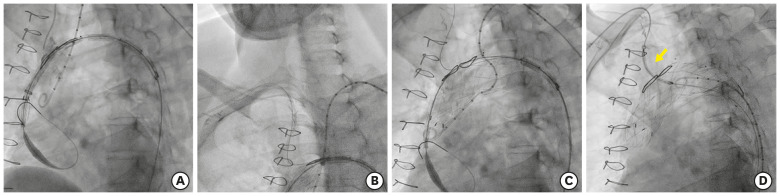
Figure 2 Main stent graft implantation procedure. (A) Sealing of aortic dissection by thoracic stent-graft 32×150 (Seal; S&G Inc., Yongin, Korea). (B) Innominate artery to right subclavian artery for snaring fenestrations (innominate artery & left common carotid artery). Five French MP-1 from right radial, 5 French Pigtail from left radial artery. (C) Main body deployment. (D) Innominate artery stentgraft implantation (yellow arrow).
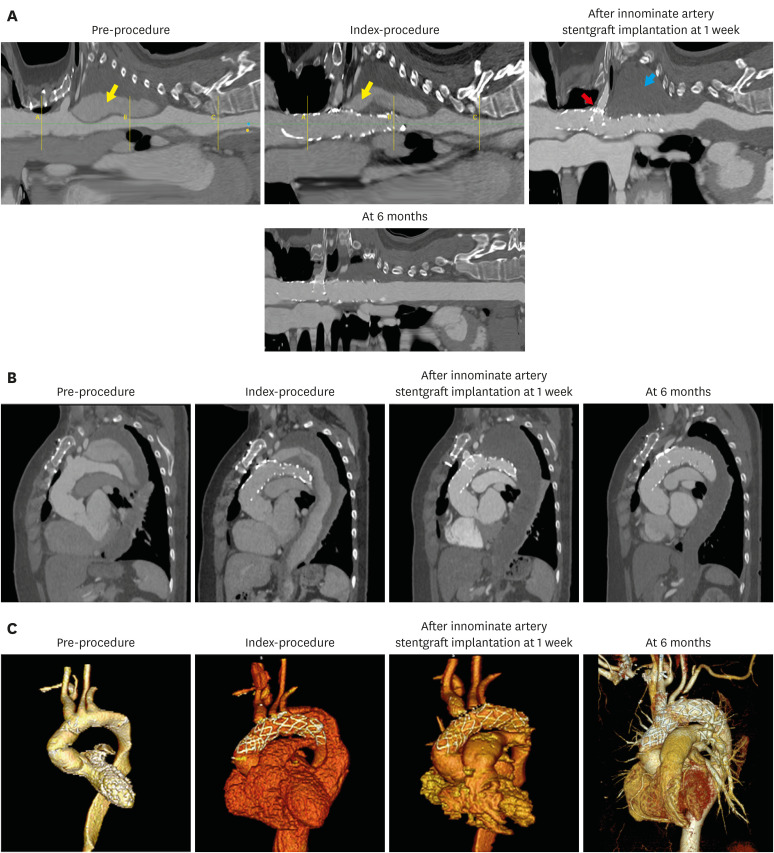
Figure 3 Serial follow-up CT showed resolution of endo-leak after stent-graft implantation. (A) Cross-sectional image. Yellow arrow: Contrast filling in false lumen, Blue arrow: Complete thrombus formation in false lumen, Red arrow: Branch stent-graft in fenestrated TEVAR. (B) Sagittal view. (C) 3D view image. Pre-procedure: Ascending aortic arch replacement status. Index-procedure: Fenestrated TEVAR with 2 fenestrae. After innominate artery stentgraft implantation at 1 week: Fenestrated TEVAR with innominate artery stent-graft.3D = 3-dimensional; CT = computerized tomography; TEVAR = thoracic endovascular aortic replacement.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Type II Aortic Dissection with Severe Aortic Regurgitation and Chronic Descending Aortic Dissection in Pregnant Patient with Marfan Syndrome
- Surgical Treatment of Acute Type A Aortic Dissection in Ehlers-Danlos Syndrome
- Endovascular Repair of Thoracic Aortic Aneurysm Using a Custom-made Fenestrated Stent Graft to Preserve the Left Subclavian Artery
- Placement of Endovascular Stent Graft in Acute Malperfusion Syndrome After Acute Type II Aortic Dissection
- Surgical Repair of Retrograde Type A Aortic Dissection after Thoracic Endovascular Aortic Repair
