Application of a traction metal clip with a fishhook-like device in wound sutures after endoscopic resection
- Affiliations
-
- 1Department of Gastroenterology, Jiangyin Hospital Affiliated to Nantong University, Jiangyin, China
- KMID: 2531946
- DOI: http://doi.org/10.5946/ce.2021.241
Abstract
- Background/Aims
Endoscopic wound suturing is an important factor that affects the ability to remove large and full-thickness lesions during endoscopic resection. We aimed to evaluate the effect of a traction metal clip with a fishhook-like device on wound sutures after endoscopic resection.
Methods
From July 2020 to April 2021, patients who met the enrollment criteria were treated with a fishhook-like device during the operation to suture the postoperative wound (group A). Patients with similar conditions and similar size wounds who were treated with a “purse-string suture” to suture the wounds were retrospectively analyzed as the control group (group B). Difference in the suture rate, adverse events, time required for suturing, and number of metal clips were compared between the two groups.
Results
The time required for suturing was 7.72±0.51 minutes in group A and 11.50±0.91 minutes in group B. This difference was statistically significant (F=13.071, p=0.001). The number of metal clamps used in group A averaged 8.1 pieces/case, and the number of metal clamps used in group B averaged 7.3 pieces/case. This difference was not statistically significant (F=0.971, p>0.05).
Conclusions
The traction metal clip with the fishhook-like device is ingeniously designed and easy to operate. It has a good suture effect on the wound after endoscopic submucosal dissection and effectively prevents postoperative adverse events.
Keyword
Figure
-

Fig. 1. Fishhook traction clip. (A) When the traction clip is opened, the fishhook-like structure can penetrate the mucosal surface. (B) When the traction clip is closed, the fishhook-like structure prevents the mucosa from falling.
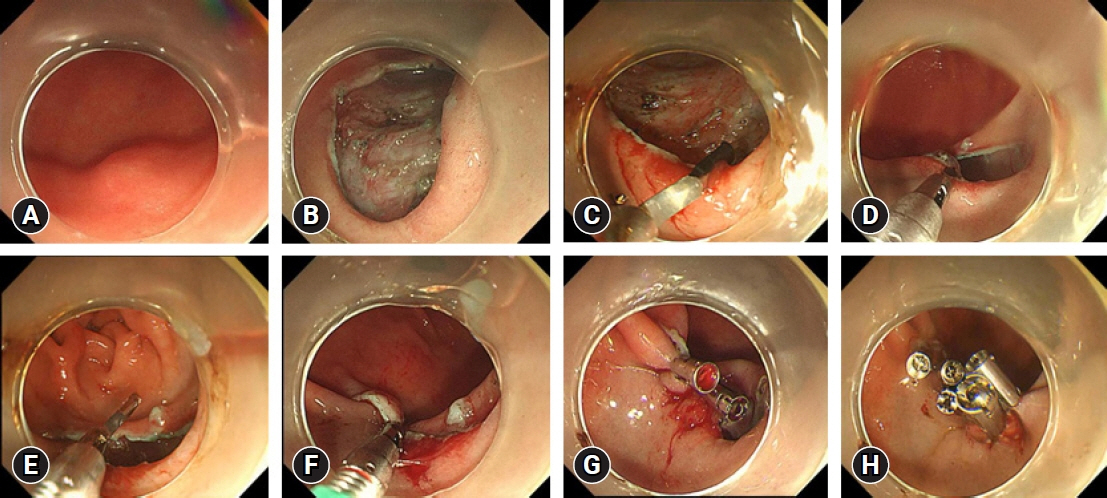
Fig. 2. The procedure of endoscopic submucosal dissection using fishhook traction clips to suture the wound. (A) A submucosal tumor on the greater curvature of the stomach, approximately 1.0×1.0 cm. (B) After removing the lesion, the wound area was approximately 2.0×3.0 cm. (C) A fishhook traction clip was used to clamp the mucosa on the side edge of the wound. (D) The mucosa was lifted so that the hook-like device penetrated the mucosa. (E) The fishhook traction clip was opened, and the mucosa was pushed from the oral side to the anal side. (F) The anal mucosa of the wound was clamped, and the wound orifice and anal side were seamed. (G) The reduced wound was sutured with ordinary metal clips. (H) The wound was sutured well.
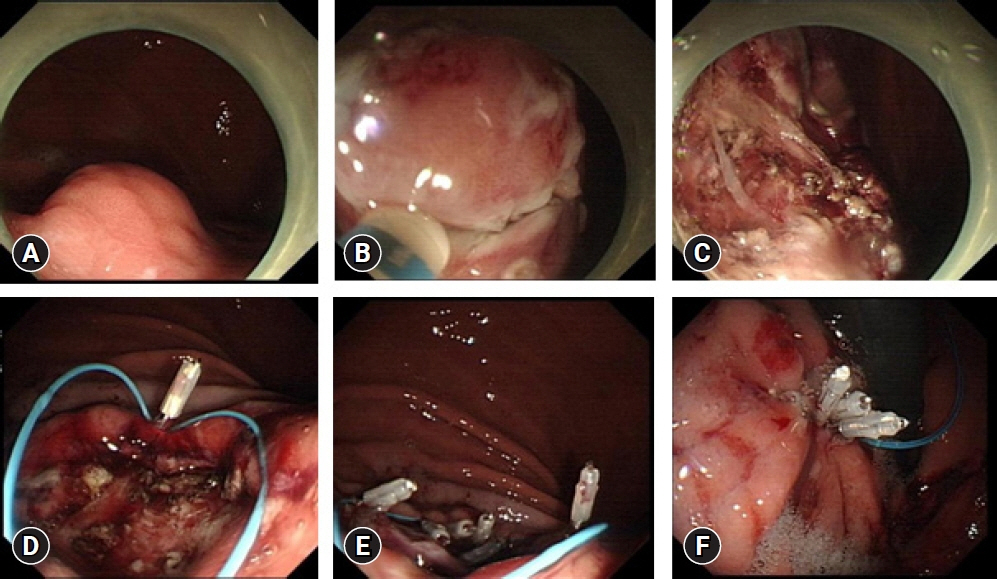
Fig. 3. The procedure of endoscopic submucosal dissection using purse-string suture. (A) A submucosal tumor about 1.8×1.5 cm in the posterior wall of the upper gastric body. (B) Make circular incision of the mucosa, expose the lesion, and peel off the tumor. (C) The wound after resection was about 2.5×3.0 cm, with 2 mm small perforations locally. (D) The first metal clip fixes the nylon rope on the distal side of the wound. (E) Use metal clips to fix the nylon rope around the wound several times. (F) Finally tighten the nylon rope to suture the wound.

Fig. 4. Box plots of observation index comparison. These four groups of data can be statistically compared, and box plots are used to compare the data more intuitively. (A) Comparison of the age of the two groups. (B) Comparison of the wound size of the two groups. (C) Comparison of the suture time of the two groups. (D) Comparison of the number of clips of the two groups.
Reference
-
1. Ono H, Yao K, Fujishiro M, et al. Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer (second edition). Dig Endosc. 2021; 33:4–20.2. Hahn KY, Park CH, Lee YK, et al. Comparative study between endoscopic submucosal dissection and surgery in patients with early gastric cancer. Surg Endosc. 2018; 32:73–86.3. Pawlak KM, Raiter A, Kozłowska-Petriczko K, et al. Optimal endoscopic resection technique for selected gastric GISTs. The endoscopic suturing system combined with ESD-a new alternative? J Clin Med. 2020; 9:1776.4. Wu N, Liu S, Chen M, et al. The prepurse-string suture technique for gastric defect after endoscopic full-thickness resection (with video). Medicine (Baltimore). 2018; 97:e12118.5. Shi Q, Chen T, Zhong YS, et al. Complete closure of large gastric defects after endoscopic full-thickness resection, using endoloop and metallic clip interrupted suture. Endoscopy. 2013; 45:329–334.6. Maekawa S, Nomura R, Murase T, et al. Complete closure of artificial gastric ulcer after endoscopic submucosal dissection by combined use of a single over-the-scope clip and through-the-scope clips (with videos). Surg Endosc. 2015; 29:500–504.7. Tang AL, Liao XQ, Shen SR, et al. Application of clips assisted with foreign body forceps in defect closure after endoscopic full-thickness resection. Surg Endosc. 2016; 30:2127–2131.8. Han S, Wani S, Kaltenbach T, et al. Endoscopic suturing for closure of endoscopic submucosal dissection defects. VideoGIE. 2019; 4:310–313.9. Kukreja K, Chennubhotla S, Bhandari B, et al. Closing the gaps: endoscopic suturing for large submucosal and full-thickness defects. Clin Endosc. 2018; 51:352–356.10. Akimoto T, Goto O, Sasaki M, et al. Endoscopic suturing promotes healing of mucosal defects after gastric endoscopic submucosal dissection: endoscopic and histologic analyses in in vivo porcine models (with video). Gastrointest Endosc. 2020; 91:1172–1182.11. Fujihara S, Mori H, Kobara H, et al. Management of a large mucosal defect after duodenal endoscopic resection. World J Gastroenterol. 2016; 22:6595–6609.12. Abe S, Saito Y, Tanaka Y, et al. A novel endoscopic hand-suturing technique for defect closure after colorectal endoscopic submucosal dissection: a pilot study. Endoscopy. 2020; 52:780–785.13. Kobayashi M, Sumiyama K, Ban Y, et al. Closure of iatrogenic large mucosal and full-thickness defects of the stomach with endoscopic interrupted sutures in in vivo porcine models: are they durable enough? BMC Gastroenterol. 2015; 15:5.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic hemostasis using an over-the-scope clip for massive bleeding after percutaneous endoscopic gastrostomy removal: a case report
- Counter Traction Makes Endoscopic Submucosal Dissection Easier
- Nipple Suspension Using Biopsy Bottle after Surgical Correction for Inverted Nipple
- Endoscopic Management with a Novel Over-The-Scope Padlock Clip System
- Review of Pure Endoscopic Full-Thickness Resection of the Upper Gastrointestinal Tract
