Clin Endosc.
2022 Jul;55(4):520-524. 10.5946/ce.2021.262.
Intralesional steroid infusion using a spray tube to prevent stenosis after endoscopic submucosal dissection of esophageal cancer
- Affiliations
-
- 1Department of Gastroenterology and Hepatology, Yamaguchi University Graduate School of Medicine, Ube, Japan
- 2Department of Gastroenterology and Hepatology, Yamaguchi Prefectural Grand Medical Center, Hofu, Japan
- 3Faculty of Laboratory Science, Yamaguchi University Graduate School of Medicine, Ube, Japan
- KMID: 2531945
- DOI: http://doi.org/10.5946/ce.2021.262
Abstract
- Background/Aims
Intralesional steroid injections have been administered as prophylaxis for stenosis after esophageal endoscopic submucosal dissection. However, this method carries a risk of potential complications such as perforation because a fine needle is used to directly puncture the postoperative ulcer. We devised a new method of steroid intralesional infusion using a spray tube and evaluated its efficacy and safety.
Methods
Intralesional steroid infusion using a spray tube was performed on 27 patients who underwent endoscopic submucosal dissection for superficial esophageal cancer with three-quarters or more of the lumen circumference resected. The presence or absence of stenosis, complications, and the number of endoscopic balloon dilations (EBDs) performed were evaluated after treatment.
Results
Although stenosis was not observed in 22 of the 27 patients, five patients had stenosis and dysphagia requiring EBD. The stenosis in these five patients was relieved after four EBDs. No complications related to intralesional steroid infusion using the spray tube were observed.
Conclusions
Intralesional steroid infusion using a spray tube is a simple and safe technique that is adequately effective in preventing stenosis Clinical trial number (UMIN000037567).
Keyword
Figure
-

Fig. 1. Spray tube (fine jet spraying type; Top Co., Tokyo, Japan).
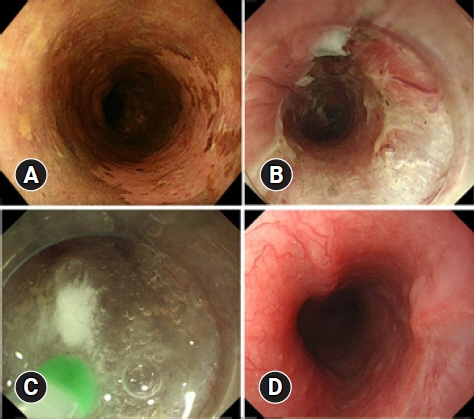
Fig. 2. (A) A patient with early esophageal cancer in the upper esophagus (patient no. 22 in Table 2). (B) Sub-circumferential resection was performed by endoscopic submucosal dissection. (C) Immediately after resection of the lesion, intralesional steroid infusion using a spray tube was performed. (D) The resected surface was completely re-epithelialized without stenosis 2 months after endoscopic submucosal dissection.
Reference
-
1. Katada C, Muto M, Manabe T, et al. Esophageal stenosis after endoscopic mucosal resection of superficial esophageal lesions. Gastrointest Endosc. 2003; 57:165–169.2. Hagel AF, Naegel A, Dauth W, et al. Perforation during esophageal dilatation: a 10-year experience. J Gastrointestin Liver Dis. 2013; 22:385–389.3. Hashimoto S, Kobayashi M, Takeuchi M, et al. The efficacy of endoscopic triamcinolone injection for the prevention of esophageal stricture after endoscopic submucosal dissection. Gastrointest Endosc. 2011; 74:1389–1393.4. Hanaoka N, Ishihara R, Takeuchi Y, et al. Intralesional steroid injection to prevent stricture after endoscopic submucosal dissection for esophageal cancer: a controlled prospective study. Endoscopy. 2012; 44:1007–1011.5. Yamaguchi N, Isomoto H, Nakayama T, et al. Usefulness of oral prednisolone in the treatment of esophageal stricture after endoscopic submucosal dissection for superficial esophageal squamous cell carcinoma. Gastrointest Endosc. 2011; 73:1115–1121.6. Ishida T, Morita Y, Hoshi N, et al. Disseminated nocardiosis during systemic steroid therapy for the prevention of esophageal stricture after endoscopic submucosal dissection. Dig Endosc. 2015; 27:388–391.7. Yamashina T, Uedo N, Fujii M, et al. Delayed perforation after intralesional triamcinolone injection for esophageal stricture following endoscopic submucosal dissection. Endoscopy. 2013; 45 Suppl 2 UCTN:E92.8. Rajan E, Gostout C, Feitoza A, et al. Widespread endoscopic mucosal resection of the esophagus with strategies for stricture prevention: a preclinical study. Endoscopy. 2005; 37:1111–1115.9. Kadota T, Yoda Y, Hori K, et al. Prophylactic steroid administration against strictures is not enough for mucosal defects involving the entire circumference of the esophageal lumen after esophageal endoscopic submucosal dissection (ESD). Esophagus. 2020; 17:440–447.10. Knyrim K, Wagner HJ, Bethge N, et al. A controlled trial of an expansile metal stent for palliation of esophageal obstruction due to inoperable cancer. N Engl J Med. 1993; 329:1302–1307.11. Yamashita S, Kato M, Fujimoto A, et al. Inadequate steroid injection after esophageal ESD might cause mural necrosis. Endosc Int Open. 2019; 7:E115–E121.12. Shibagaki K, Ishimura N, Oshima N, et al. Esophageal triamcinolone acetonide-filling method: a novel procedure to prevent stenosis after extensive esophageal endoscopic submucosal dissection (with videos). Gastrointest Endosc. 2018; 87:380–389.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prevention of stricture after endoscopic submucosal dissection for esophageal cancer: intralesional steroid infusion using a spray tube
- Intralesional Steroid Injection to Prevent Stricture after Near-Circumferential Endosopic Submucosal Dissection for Superficial Esophageal Cancer
- Endoscopic Submucosal Dissection Followed by Concurrent Chemoradiotherapy in Patients with Early Esophageal Cancer with a High Risk of Lymph Node Metastasis
- Endoscopic Treatment for Esophageal Cancer
- Iatrogenic Esophageal Submucosal Dissection: A Case Report
