Transradial Approach for Thoracolumbar Spinal Angiography and Tumor Embolization: Feasibility and Technical Considerations
- Affiliations
-
- 1Department of Neurointerventional Radiology, University of California San Francisco, San Francisco, CA, USA
- 2Department of Neurological Surgery, University of California San Francisco, San Francisco, CA, USA
- KMID: 2531565
- DOI: http://doi.org/10.5469/neuroint.2022.00010
Abstract
- The transradial approach (TRA) is an effective and safe alternative to transfemoral access for diagnostic neuroangiography and craniocervical interventions. While the technical aspects of supraclavicular intervention are well-described, there are little data on the TRA for thoracolumbar angiography and intervention. The authors describe the feasibility of the TRA for preoperative thoracic tumor embolization, emphasizing technique, device selection, navigation, and catheterization of thoracolumbar segmental arteries. This approach extends the benefits of TRA to spinal interventional neuroradiology.
Keyword
Figure
-
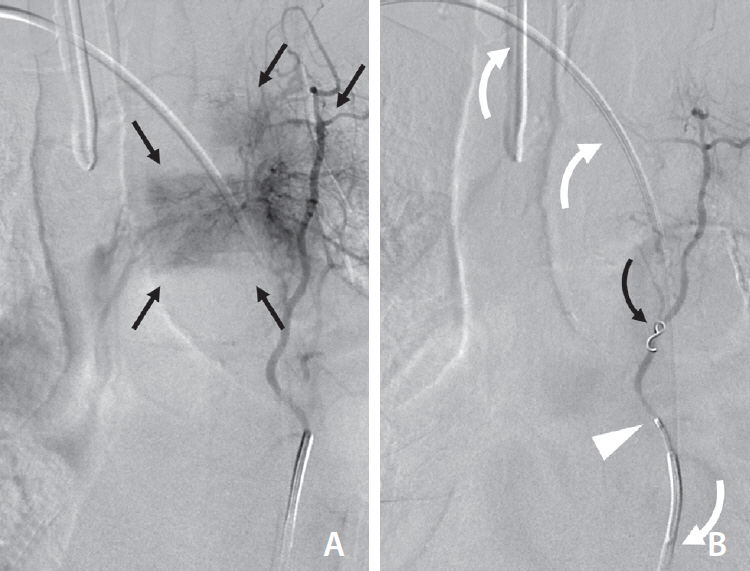
Fig. 1. (A) Digital subtraction angiography selective injection of the left T3 segmental artery through the diagnostic catheter demonstrates cranial angulation and hypervascular tumor blush (black straight arrows) involving the T3 vertebral body and adjacent soft tissues. (B) Post-embolization selective injection through the microcatheter (white arrowhead) shows significantly reduced tumor vascularity with intra-arterial coil placement (curved black arrow). The course of the Simmons-type catheter from the trans-radial approach is demonstrated by curved white arrows.
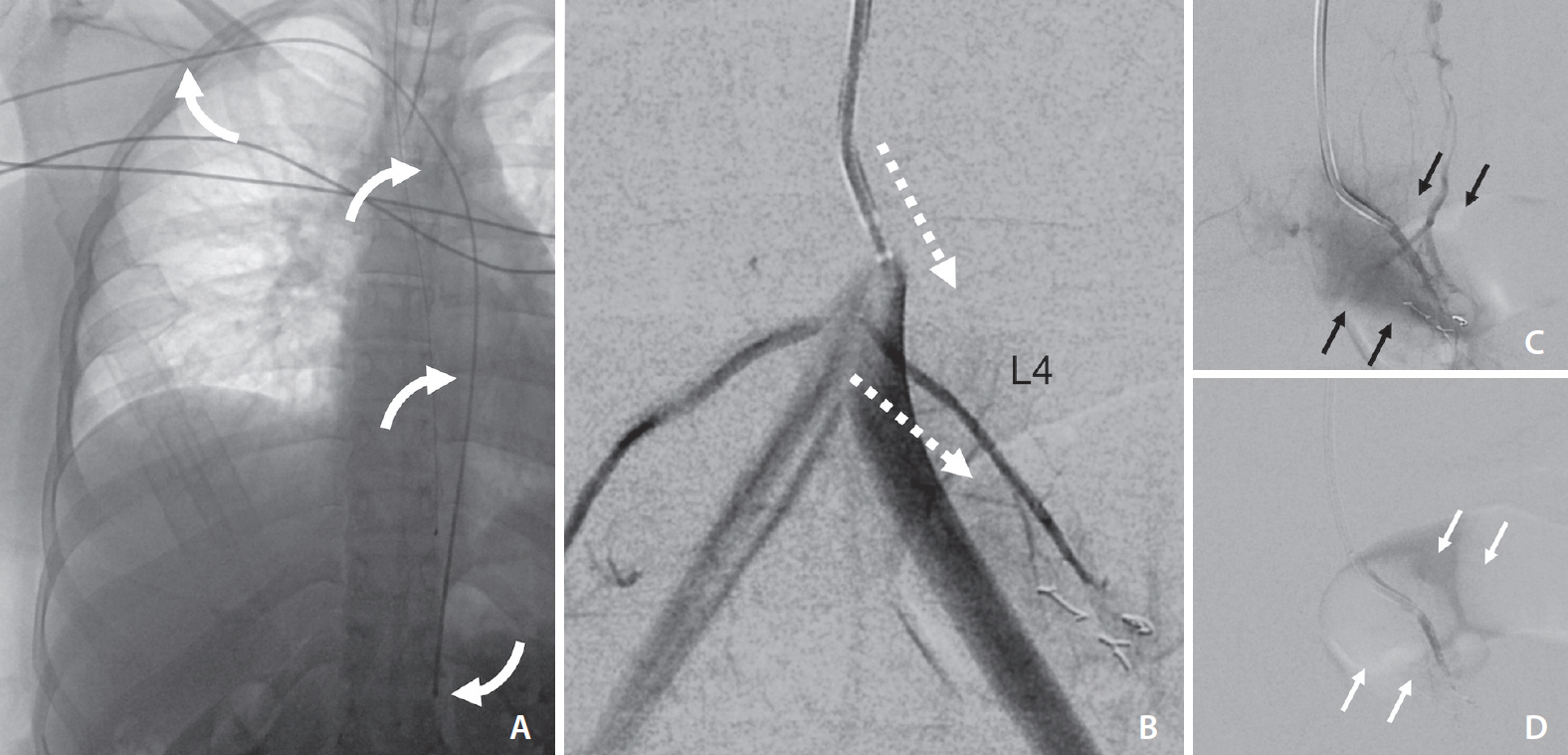
Fig. 2. TRA using long (130 cm) Penumbra Vert Catheter (A, white curved arrows). DSA roadmap (B) shows near parallel orientation of the left L4 segmental artery origin and the catheter tip angle (white dotted arrows). Over a glidewire, the catheter could easily select the segmental artery (C, tumor blush=black arrows), facilitating successful repeat embolization using PVA particles (D, post-embolization, diminished tumor blush=white arrows). TRA, transradial approach; DSA, digital subtraction angiography; PVA, polyvinyl alcohol.

Fig. 3. Summary of “inverse” catheter geometry and strategies for spinal radicular artery selection with 4 common aortic catheter types. The Simmons-type catheter (A) was used to access the left T3 segmental artery and may be favorable for many upper and mid-thoracic lesions. The C2 (“Cobra”) catheter (B) has a cranially-directed tip which may be advantageous for upper thoracic segmental arteries. The Vertebral catheter shape (C) affords less support in the aorta lumen but may be optimal for caudally-directed lumbar segmental arteries. The Mikaelsson catheter (D) offers the most “neutral” tip-angle and would therefore function similarly from transradial and transfemoral approaches, providing the greatest stability at mid-thoracic levels.
Reference
-
1. Wilson MA, Cooke DL, Ghodke B, Mirza SK. Retrospective analysis of preoperative embolization of spinal tumors. AJNR Am J Neuroradiol. 2010; 31:656–660.
Article2. Prabhu VC, Bilsky MH, Jambhekar K, Panageas KS, Boland PJ, Lis E, et al. Results of preoperative embolization for metastatic spinal neoplasms. Neurosurg. 2003; 98(2 Suppl):156–164.
Article3. Gellad FE, Sadato N, Numaguchi Y, Levine AM. Vascular metastatic lesions of the spine: preoperative embolization. Radiology. 1990; 176:683–686.
Article4. Griessenauer CJ, Salem M, Hendrix P, Foreman PM, Ogilvy CS, Thomas AJ. Preoperative embolization of spinal tumors: a systematic review and meta-analysis. World Neurosurg. 2016; 87:362–371.
Article5. Gailloud P. Introduction to diagnostic and therapeutic spinal angiography. Neuroimaging Clin N Am. 2019; 29:595–614.
Article6. Narsinh KH, Mirza MH, Duvvuri M, Caton MT Jr, Baker A, Winkler EA, et al. Radial artery access anatomy: considerations for neuroendovascular procedures. J Neurointerv Surg. 2021; 13:1139–1144.
Article7. Narsinh KH, Mirza MH, Caton MT Jr, Baker A, Winkler E, Higashida RT, et al. Radial artery access for neuroendovascular procedures: safety review and complications. J Neurointerv Surg. 2021; 13:1132–1138.
Article8. Haynes J, Nossek E, Shapiro M, Chancellor B, Frempong-Boadu A, Peschillo S, et al. Radial arterial access for thoracic intraoperative spinal angiography in the prone position. World Neurosurg. 2020; 137:e358–e365.
Article9. Kühn AL, de Macedo Rodrigues K, Singh J, Massari F, Puri AS. Distal radial access in the anatomical snuffbox for neurointerventions: a feasibility, safety, and proof-of-concept study. J Neurointerv Surg. 2020; 12:798–801.
Article10. Orru E, Tsang COA, Klostranec JM, Pereira VM. Republished: transradial approach in the treatment of a sacral dural arteriovenous fistula: a technical note. J Neurointerv Surg. 2019; 11:e4.
Article11. Knox JA, Alexander MD, McCoy DB, Murph DC, Hinckley PJ, Ch’ang JC, et al. Impact of aortic arch anatomy on technical performance and clinical outcomes in patients with acute ischemic stroke. AJNR Am J Neuroradiol. 2020; 41:268–273.
Article12. Luo N, Qi W, Tong W, Meng B, Feng W, Zhou X, et al. The effect of vascular morphology on selective left vertebral artery catheterization in right-sided radial artery cerebral angiography. Ann Vasc Surg. 2019; 56:62–72.
Article13. Hacein-Bey L, Konstas AA, Pile-Spellman J. Natural history, current concepts, classification, factors impacting endovascular therapy, and pathophysiology of cerebral and spinal dural arteriovenous fistulas. Clin Neurol Neurosurg. 2014; 121:64–75.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Feasibility and Problems in Transradial Coronary Angiography and Intervention
- The Safety and Feasibility of Transradial Coronary Angiography Over 70-Year-Old Patients
- Percutaneous Transradial Approach for Coronary Angiography
- Is Transradial Cerebral Angiography Feasible and Safe? A Single Center's Experience
- A Case of Transradial Approach to Carotid Artery Angioplasty and Stenting in Left Internal Carotid Stenosis
