The Clinical Impact of β-Blocker Therapy on Patients With Chronic Coronary Artery Disease After Percutaneous Coronary Intervention
- Park J
 1
1 - Han JK1
- Kang J1
- Chae IH2
- Lee SY3
- Choi YJ4
- Rhew JY5
- Rha SW6
- Shin ES7
- Woo SI8
- Lee HC9
- Chun KJ10
- Kim D11
- Jeong JO12
- Bae JW13
- Yang HM1
- Park KW1
- Kang HJ1
- Koo BK1
- Kim HS1
- Affiliations
-
- 1Cardiovascular Center, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
- 2Cardiovascular Center, Seoul National University Bundang Hospital, Seongnam, Korea
- 3Department of Internal Medicine, Inje University Ilsan Paik Hospital, Goyang, Korea
- 4Department of Internal Medicine, Sejong General Hospital, Bucheon, Korea
- 5Department of Internal Medicine and Cardiovascular Center, Presbyterian Medical Center, Jeonju, Korea
- 6Cardiovascular Center, Korea University Guro Hospital, Seoul, Korea
- 7Department of Cardiology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea
- 8Department of Internal Medicine, Inha University Hospital, Incheon, Korea
- 9Department of Internal Medicine, Pusan National University Hospital, Busan, Korea
- 10Department of Internal Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea
- 11Department of Internal Medicine, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea
- 12Department of Internal Medicine, Chungnam National University College of Medicine, Daejeon, Korea
- 13Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea
- KMID: 2530736
- DOI: http://doi.org/10.4070/kcj.2021.0395
Abstract
- Background and Objectives
The outcome benefits of β-blockers in chronic coronary artery disease (CAD) have not been fully assessed. We evaluated the prognostic impact of β-blockers on patients with chronic CAD after percutaneous coronary intervention (PCI).
Methods
A total of 3,075 patients with chronic CAD were included from the Grand DrugEluting Stent registry. We analyzed β-blocker prescriptions, including doses and types, in each patient at 3-month intervals from discharge. After propensity score matching, 1,170 pairs of patients (β-blockers vs. no β-blockers) were derived. Primary outcome was defined as a composite endpoint of all-cause death and myocardial infarction (MI). We further analyzed the outcome benefits of different doses (low-, medium-, and high-dose) and types (conventional or vasodilating) of β-blockers.
Results
During a median (interquartile range) follow-up of 3.1 (3.0–3.1) years, 134 (5.7%) patients experienced primary outcome. Overall, β-blockers demonstrated no significant benefit in primary outcome (hazard ratio [HR], 0.88; 95% confidence interval [CI], 0.63–1.24), all-cause death (HR, 0.87; 95% CI, 0.60–1.25), and MI (HR, 1.25; 95% CI, 0.49–3.15). In subgroup analysis, β-blockers were associated with a lower risk of all-cause death in patients with previous MI and/ or revascularization (HR, 0.38; 95% CI, 0.14–0.99) (p for interaction=0.045). No significant associations were found for the clinical outcomes with different doses and types of β-blockers.
Conclusions
Overall, β-blocker therapy was not associated with better clinical outcomes in patients with chronic CAD undergoing PCI. Limited mortality benefit of β-blockers may exist for patients with previous MI and/or revascularization.
Figure
-

Figure 1 Study flow.A total of 17,286 patients with CAD who had undergone PCI were screened for inclusion from the Grand-DES multi-center registry. We excluded patients whose prescription records of β-blockers were not available and those with non-continuous use of β-blockers during the follow-up period. Finally, a total of 3,075 patients with chronic CAD were included. After propensity score matching, a total of 1,170 pairs of patients were finally derived.CAD = coronary artery disease; DES = drug-eluting stent; PCI = percutaneous coronary intervention; PS = propensity score.
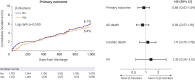
Figure 2 Clinical outcomes according to β-blocker therapy in matched population.Among the matched population, the β-blocker group was not associated with better clinical outcomes in primary outcome, all-cause death, cardiac death, and MI compared with the no β-blocker group.CI = confidence interval; HR = hazard ratio; MI = myocardial infarction.

Figure 3 Subgroup analysis for primary outcome and all-cause death associated with β-blocker therapy.There was no significant difference in primary outcome associated with β-blocker therapy across the various subgroups. β-blockers were associated with a lower risk of all-cause death in patients with previous MI and/or revascularization.BES = Biolimus A9 eluting coronary stent; CHF = congestive heart failure; CI = confidence interval; DAPT = dual antiplatelet therapy; DES = drug-eluting stent; EES = Everolimus eluting coronary stent; HR = hazard ratio; LVEF = left ventricular ejection fraction; MI = myocardial infarction; ZES = Zotarolimus eluting coronary stent.
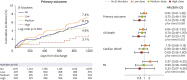
Figure 4 Clinical outcomes according to different doses of β-blockers.After dose stratification, there was a dose-dependent tendency of lower risk of mortality with higher β-blockers doses, although the result was not statistically significant.CI = confidence interval; HR = hazard ratio; MI = myocardial infarction.
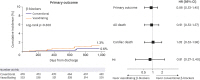
Figure 5 Clinical outcomes according to different types of β-blockers.Compared with patients who received conventional β-blockers, those with vasodilating β-blockers were not associated with better clinical outcomes.CI = confidence interval; HR = hazard ratio; MI = myocardial infarction.
Cited by 1 articles
-
Role of β-Blockers in Chronic Coronary Artery Disease Management in the Percutaneous Coronary Intervention Era: Good Symptom Control or Something More?
Ji Woong Roh, Yongcheol Kim
Korean Circ J. 2022;52(7):556-557. doi: 10.4070/kcj.2022.0105.
Reference
-
1. Dargie HJ. Effect of carvedilol on outcome after myocardial infarction in patients with left-ventricular dysfunction: the CAPRICORN randomised trial. Lancet. 2001; 357:1385–1390. PMID: 11356434.
Article2. Puymirat E, Riant E, Aissaoui N, et al. β blockers and mortality after myocardial infarction in patients without heart failure: multicentre prospective cohort study. BMJ. 2016; 354:i4801. PMID: 27650822.
Article3. Dahl Aarvik M, Sandven I, Dondo TB, et al. Effect of oral β-blocker treatment on mortality in contemporary post-myocardial infarction patients: a systematic review and meta-analysis. Eur Heart J Cardiovasc Pharmacother. 2019; 5:12–20. PMID: 30192930.
Article4. Hwang D, Lee JM, Kim HK, et al. Prognostic impact of β-blocker dose after acute myocardial infarction. Circ J. 2019; 83:410–417. PMID: 30464110.
Article5. Packer M, Coats AJ, Fowler MB, et al. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med. 2001; 344:1651–1658. PMID: 11386263.
Article6. Leizorovicz A, Lechat P, Cucherat M, Bugnard F. Bisoprolol for the treatment of chronic heart failure: a meta-analysis on individual data of two placebo-controlled studies--CIBIS and CIBIS II. Cardiac Insufficiency Bisoprolol Study. Am Heart J. 2002; 143:301–307. PMID: 11835035.
Article7. Andersson C, Shilane D, Go AS, et al. β-Blocker therapy and cardiac events among patients with newly diagnosed coronary heart disease. J Am Coll Cardiol. 2014; 64:247–252. PMID: 25034059.
Article8. Bangalore S, Steg G, Deedwania P, et al. β-Blocker use and clinical outcomes in stable outpatients with and without coronary artery disease. JAMA. 2012; 308:1340–1349. PMID: 23032550.
Article9. Motivala AA, Parikh V, Roe M, et al. Predictors, trends, and outcomes (among older patients ≥65 years of age) associated with beta-blocker use in patients with stable angina undergoing elective percutaneous coronary intervention: insights from the NCDR registry. JACC Cardiovasc Interv. 2016; 9:1639–1648. PMID: 27539683.
Article10. Hjalmarson A, Elmfeldt D, Herlitz J, et al. Effect on mortality of metoprolol in acute myocardial infarction. A double-blind randomised trial. Lancet. 1981; 2:823–827. PMID: 6116950.11. Johnston DL, Gebhardt VA, Donald A, Kostuk WJ. Comparative effects of propranolol and verapamil alone and in combination on left ventricular function and volumes in patients with chronic exertional angina: a double-blind, placebo-controlled, randomized, crossover study with radionuclide ventriculography. Circulation. 1983; 68:1280–1289. PMID: 6315259.
Article12. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial. Lancet. 1999; 353:9–13. PMID: 10023943.13. Viskin S, Kitzis I, Lev E, et al. Treatment with beta-adrenergic blocking agents after myocardial infarction: from randomized trials to clinical practice. J Am Coll Cardiol. 1995; 25:1327–1332. PMID: 7722129.
Article14. Ambrosio G, Flather MD, Böhm M, et al. β-blockade with nebivolol for prevention of acute ischaemic events in elderly patients with heart failure. Heart. 2011; 97:209–214. PMID: 21138861.
Article15. Narahara KA. Betaxolol Investigators Group. Double-blind comparison of once daily betaxolol versus propranolol four times daily in stable angina pectoris. Am J Cardiol. 1990; 65:577–582. PMID: 2178381.
Article16. Rodrigues EA, Lawrence JD, Dasgupta P, et al. Comparison of bevantolol and atenolol in chronic stable angina. Am J Cardiol. 1988; 61:1204–1209. PMID: 2897780.
Article17. Sorbets E, Steg PG, Young R, et al. β-Blockers, calcium antagonists, and mortality in stable coronary artery disease: an international cohort study. Eur Heart J. 2019; 40:1399–1407. PMID: 30590529.
Article18. Goldberger JJ, Bonow RO, Cuffe M, et al. Effect of beta-blocker dose on survival after acute myocardial infarction. J Am Coll Cardiol. 2015; 66:1431–1441. PMID: 26403339.
Article19. Park J, Han JK, Kang J, et al. Optimal dose and type of β-blockers in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Am J Cardiol. 2020; 137:12–19. PMID: 32998005.
Article20. Parsons LS. Reducing bias in a propensity score matched-pair sample using greedy matching techniques. In : Proceedings of the Twenty-Sixth Annual SAS Users Group International Conference; 2001 Apr 22-25; Long Beach, CA. place unknown: SAS User Groups;2001.21. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009; 28:3083–3107. PMID: 19757444.
Article22. Bangalore S, Bhatt DL, Steg PG, et al. β-Blockers and cardiovascular events in patients with and without myocardial infarction: post hoc analysis from the CHARISMA trial. Circ Cardiovasc Qual Outcomes. 2014; 7:872–881. PMID: 25271049.
Article23. Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020; 41:407–477. PMID: 31504439.24. Diaz A, Bourassa MG, Guertin MC, Tardif JC. Long-term prognostic value of resting heart rate in patients with suspected or proven coronary artery disease. Eur Heart J. 2005; 26:967–974. PMID: 15774493.
Article25. Bangalore S, Makani H, Radford M, et al. Clinical outcomes with β-blockers for myocardial infarction: a meta-analysis of randomized trials. Am J Med. 2014; 127:939–953. PMID: 24927909.
Article26. Fonseca VA. Effects of beta-blockers on glucose and lipid metabolism. Curr Med Res Opin. 2010; 26:615–629. PMID: 20067434.27. Chung J, Han JK, Kim YJ, et al. Benefit of vasodilating β-blockers in patients with acute myocardial infarction after percutaneous coronary intervention: nationwide multicenter cohort study. J Am Heart Assoc. 2017; 6:e007063. PMID: 29066446.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent Advances in Percutaneous Coronary Intervention in Coronary Artery Disease
- Diffuse Long Coronary Artery Disease is Still an Obstacle for Percutaneous Coronary Intervention in the Second-Generation Drug-Eluting Stent Era?
- Diabetes Mellitus and Coronary Angiography
- The Prognostic Impact of Hypertriglyceridemia and Abdominal Obesity in Acute Myocardial Infarction Patients Underwent Percutaneous Coronary Intervention
- Percutaneous transluminal coronary angioplasty for ostial stenosis of the left coronary artery
