Current Trends in the Treatment of Syndesmotic Injury: Analysis of the Korean Foot and Ankle Society (KFAS) Member Survey
- Affiliations
-
- 1Department of Orthopedic Surgery, Hallym University Chuncheon Sacred Heart Hospital, Chuncheon, Korea
- 2Department of Orthopedic Surgery, Chungbuk National University Hospital, Cheongju, Korea
- 3Department of Orthopaedic Surgery, College of Medicine, Kyung Hee University, Seoul, Korea
- 4Department of Orthopedic Surgery, The Catholic University of Korea, Bucheon St. Mary’s Hospital, Bucheon, Korea
- 5Department of Orthopedic Surgery, Inje University Sanggye Paik Hospital, Seoul, Korea
- KMID: 2530490
- DOI: http://doi.org/10.14193/jkfas.2022.26.2.95
Abstract
- Purpose
This study was based on the Korean Foot and Ankle Society (KFAS) member survey and aimed to report the current trends in the management of syndesmotic injuries over the last few decades.
Materials and Methods
A web-based questionnaire containing 36 questions was sent to all KFAS members in September 2021. The questions were mainly related to the preferred techniques and clinical experiences in the treatment of patients with syndesmotic injuries. Answers with a prevalence ≥50% of respondents were considered a tendency.
Results
Seventy-six (13.8%) of the 550 members responded to the survey. The results showed that the most preferred method to diagnose a syndesmotic injury was magnetic resonance imaging (MRI). Intraoperatively, the external rotation stress test and the Cotton test were most frequently used to confirm syndesmotic diastasis. The reduction was usually done by a reduction clamp. One 3.5-mm screw was used most frequently over three cortices at 2~4 cm above the ankle joint. The preferred ankle position during fixation was 0° dorsiflexion. Removal of the syndesmotic screw was routinely done by most surgeons, mainly because of the limitation of movement and risk of screw breakage. Factors that affect suture button selection included non-rigid fixation which enables adequate fixation, early weight-bearing, and an infrequent need to remove the hardware. Inadequate reduction was considered the main factor that affects poor prognosis.
Conclusion
This study proposes updated information about the current trends in the management of syndesmotic injuries in Korea. Consensuses in both the diagnostic and therapeutic approach to patients with syndesmotic injury were identified in this survey study. This study may raise the awareness of the various possible approaches toward the injury and should be used to further establish a standard protocol for the management of syndesmotic injuries.
Keyword
Figure
-

Figure. 1 Preferred method to diagnose syndesmotic injury (choose up to 3). MRI: magnetic resonance imaging, CT: computed tomography.
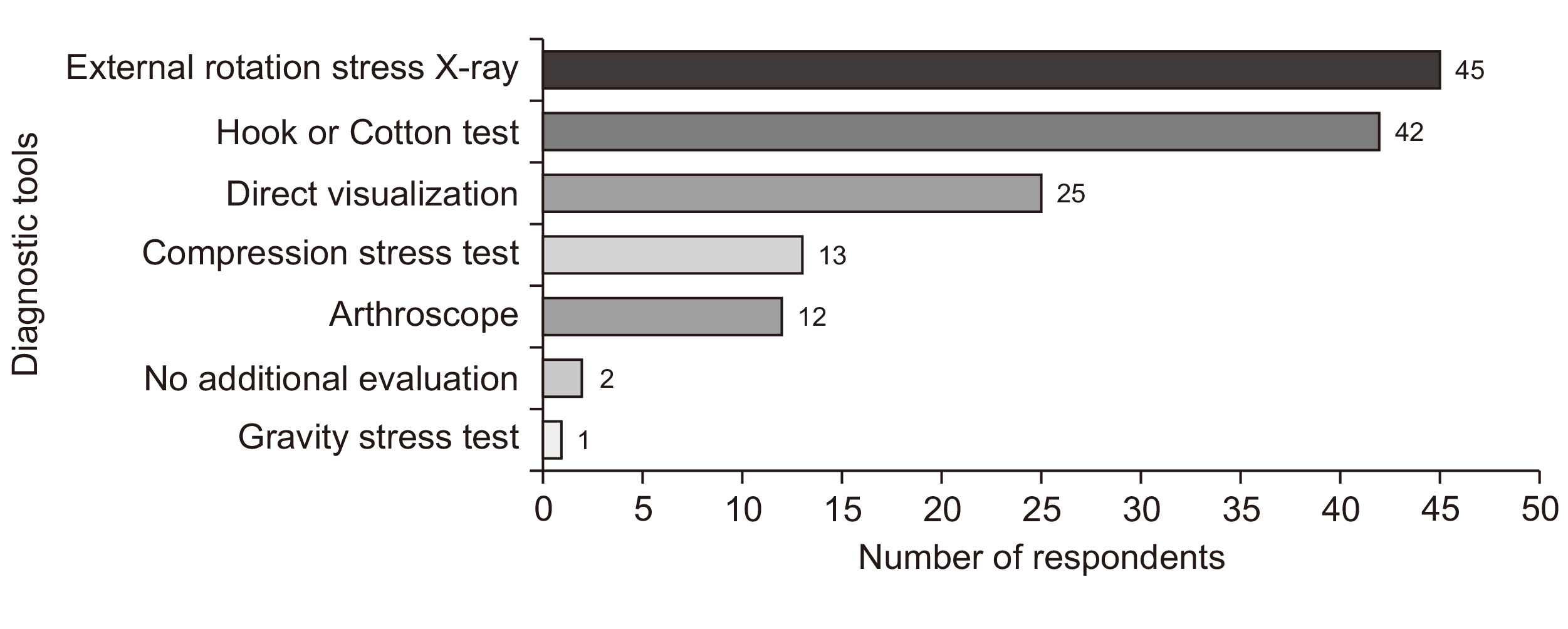
Figure. 2 Preferred intra-operative diagnostic method to diagnose syndesmotic diastasis (choose up to 2).
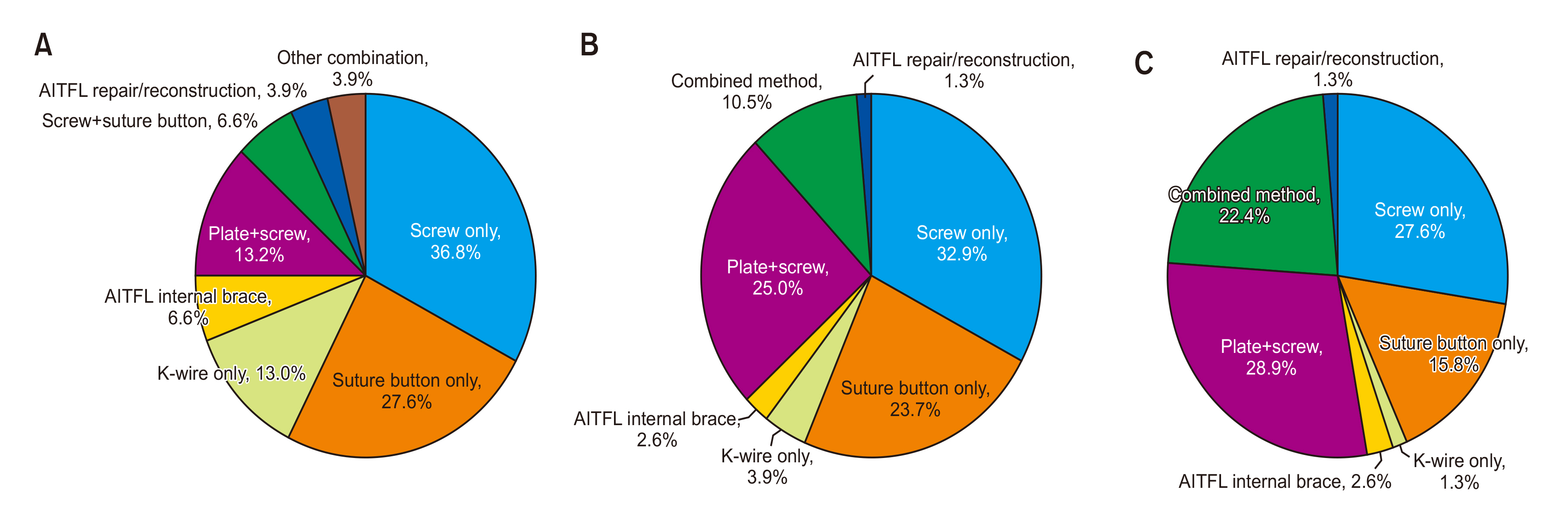
Figure. 3 Preferred fixation device syndesmotic injury. (A) Without ankle fracture; (B) with ankle fracture; (C) Maisonneuve fracture. AITFL: anterior inferior tibiofibular ligament.
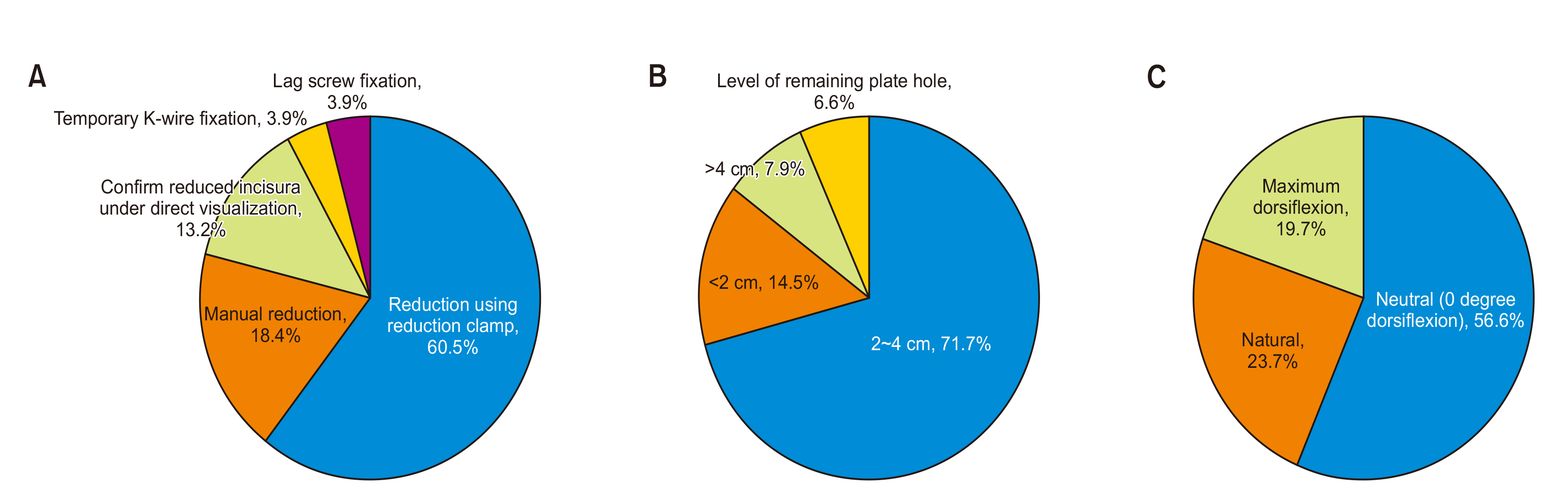
Figure. 4 Preferred reduction and fixation methods. (A) Reduction method, (B) fixation level (proximal from ankle joint), (C) ankle position during fixation.
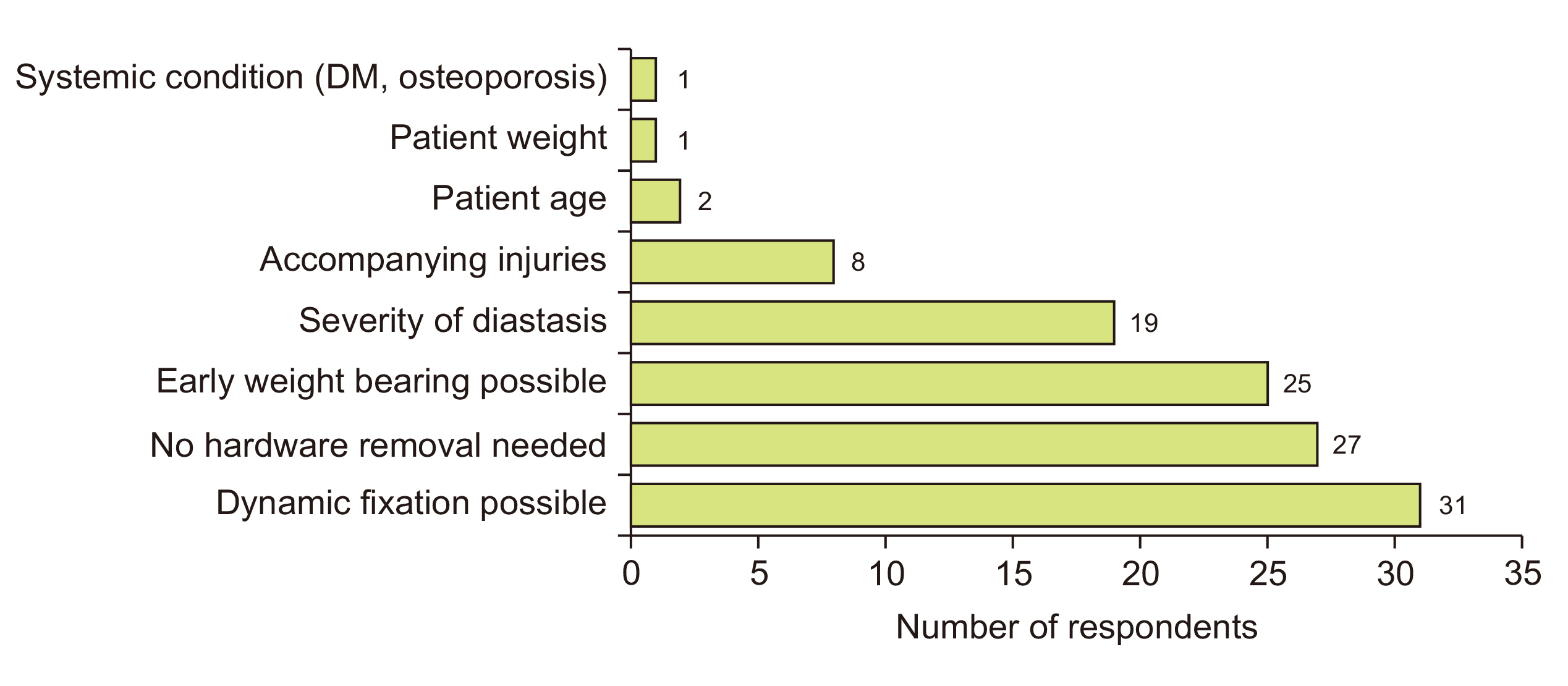
Figure. 5 Factors to select suture button fixation (choose up to 3). DM: diabetes mellitus.
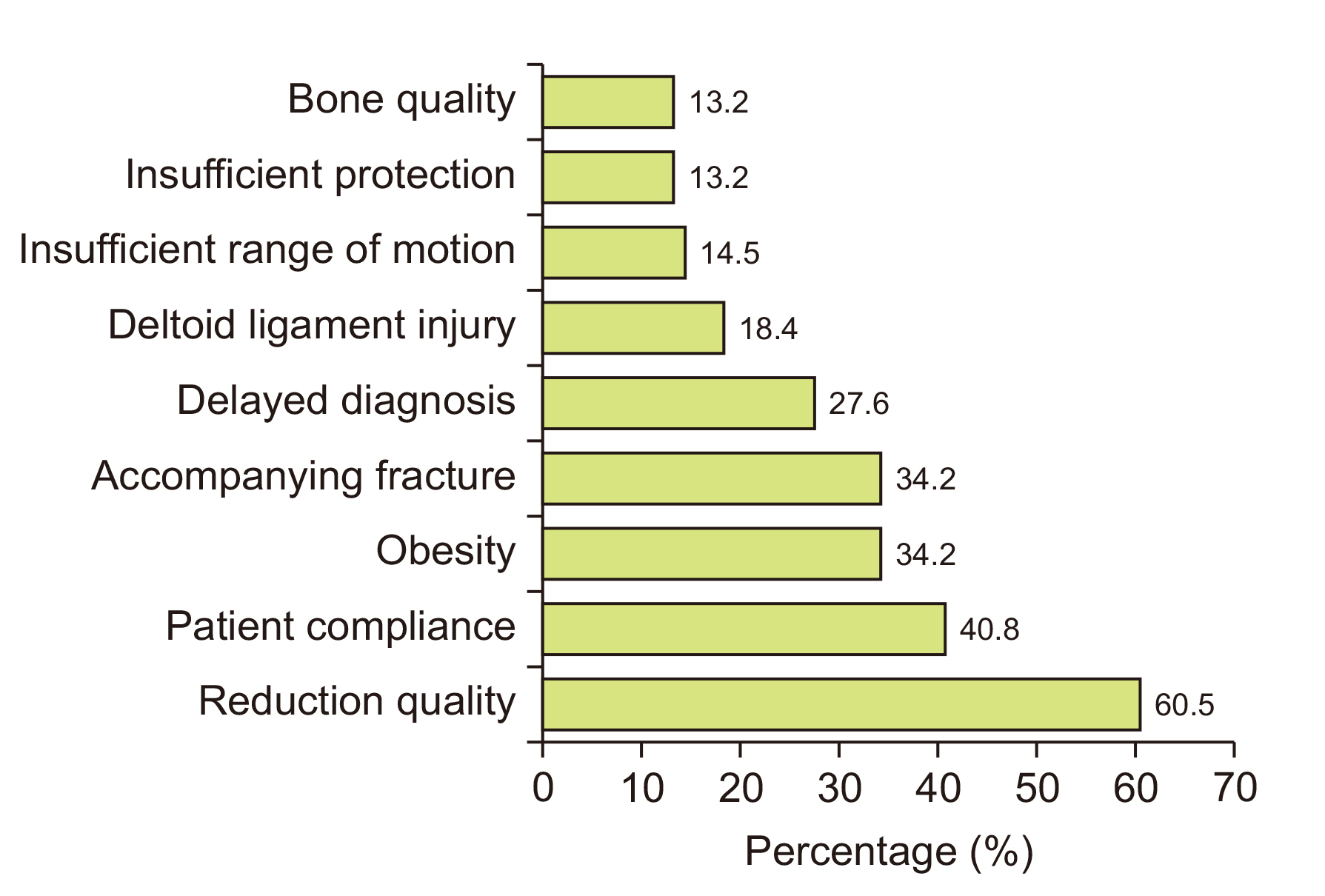
Figure. 6 Factors that affect poor prognosis (choose up to 3).
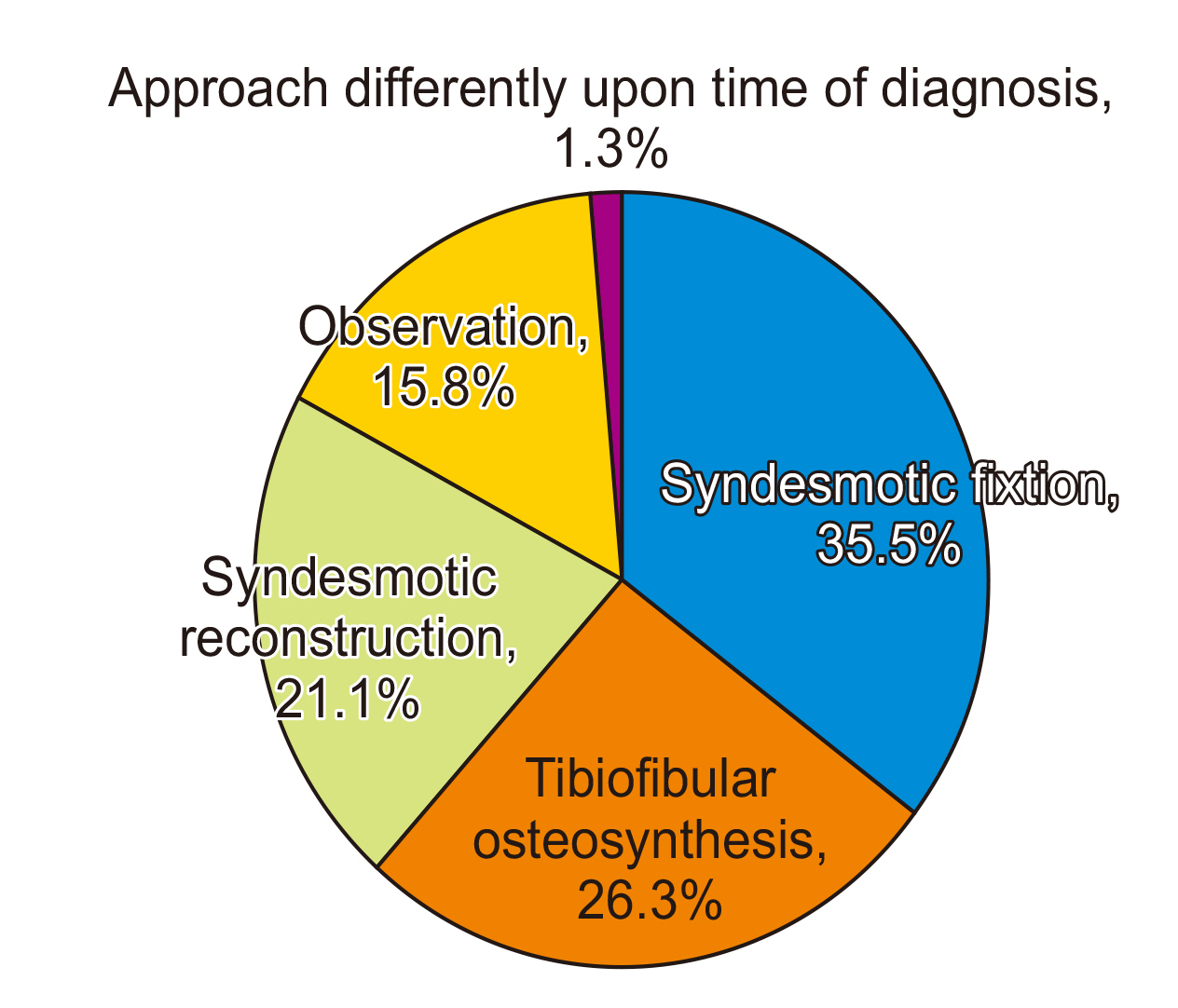
Figure. 7 Treatment for a neglected syndesmotic injury.
Reference
-
1. Chun DI, Cho JH, Min TH, Park SY, Kim KH, Kim JH, et al. 2019; Diagnostic accuracy of radiologic methods for ankle syndesmosis injury: a systematic review and meta-analysis. J Clin Med. 8:968. doi: 10.3390/jcm8070968. DOI: 10.3390/jcm8070968. PMID: 31277316. PMCID: PMC6678834.
Article2. Ræder BW, Figved W, Madsen JE, Frihagen F, Jacobsen SB, Andersen MR. Better outcome for suture button compared with single syndesmotic screw for syndesmosis injury: five-year results of a randomized controlled trial. Bone Joint J. 2020; 102-B:212–9. doi: 10.1302/0301-620X.102B2.BJJ-2019-0692.R2. DOI: 10.1302/0301-620X.102B2.BJJ-2019-0692.R2. PMID: 32009435.
Article3. Schnetzke M, Vetter SY, Beisemann N, Swartman B, Grützner PA, Franke J. 2016; Management of syndesmotic injuries: what is the evidence? World J Orthop. 7:718–25. doi: 10.5312/wjo.v7.i11.718. DOI: 10.5312/wjo.v7.i11.718. PMID: 27900268. PMCID: PMC5112340.
Article4. Paez CJ, Lurie BM, Upasani VV, Pennock AT. 2021; Functional outcomes of unstable ankle fractures with and without syndesmotic fixation in the adolescent population. J Child Orthop. 15:418–25. doi: 10.1302/1863-2548.15.200250. DOI: 10.1302/1863-2548.15.200250. PMID: 34476034. PMCID: PMC8381395.
Article5. Weerasekara I, Osmotherly PG, Snodgrass S, Tessier J, Rivett DA. 2021; Is the fibula positioned anteriorly in weight-bearing in individuals with chronic ankle instability? A case control study. J Man Manip Ther. 29:168–75. doi: 10.1080/10669817.2020.1844852. DOI: 10.1080/10669817.2020.1844852. PMID: 33185146. PMCID: PMC8183527.
Article6. Carr JC 2nd, Werner BC, Yarboro SR. 2016; An update on management of syndesmosis injury: a national US database study. Am J Orthop (Belle Mead NJ). 45:E472–7. PMID: 28005114.7. Nielson JH, Gardner MJ, Peterson MG, Sallis JG, Potter HG, Helfet DL, et al. Radiographic measurements do not predict syndesmotic injury in ankle fractures: an MRI study. Clin Orthop Relat Res. 2005; (436):216–21. doi: 10.1097/01.blo.0000161090.86162.19. DOI: 10.1097/01.blo.0000161090.86162.19. PMID: 15995444.8. Lim SK, Ho YC, Ling SK, Yung PS. 2021; Functional outcome of fusion versus ligament reconstruction in patients with a syndesmosis injury: a narrative review. Asia Pac J Sports Med Arthrosc Rehabil Technol. 25:53–9. doi: 10.1016/j.asmart.2021.05.002. Erratum in: Asia Pac J Sports Med Arthrosc Rehabil Technol. 2021;26:58. DOI: 10.1016/j.asmart.2021.05.002. PMID: 34195011. PMCID: PMC8215136.
Article9. Atilla HA, Öztürk A, Bilgetekin YG, Aslan H, Akkurt MO, Akdoğan M. 2020; Is there any change in surgeon's attitude to the management of ankle fractures accompanying syndesmotic injury? A nationwide survey. Jt Dis Relat Surg. 31:548–56. doi: 10.5606/ehc.2020.75527. DOI: 10.5606/ehc.2020.75527. PMID: 32962588. PMCID: PMC7607959.
Article10. González-Lucena G, Pérez-Prieto D, López-Alcover A, Ginés-Cespedosa A. 2018; Ankle fracture controversies: do the foot and ankle specialists have a different vision? Rev Esp Cir Ortop Traumatol (Engl Ed). 62:27–34. doi: 10.1016/j.recot.2017.10.001. DOI: 10.1016/j.recot.2017.10.001. PMID: 29162365.
Article11. Rogero RG, Illical EM, Corr DO, Raikin SM, Krieg JC, Tsai J. 2021; Management of ankle fractures with syndesmotic disruption: a survey of orthopaedic surgeons. Cureus. 13:e16391. doi: 10.7759/cureus.16391. DOI: 10.7759/cureus.16391. PMID: 34408944. PMCID: PMC8363056.
Article12. Shafiq H, Iqbal Z, Khan MNH, Rasool MU, Faraz A, Jamshed MH, et al. 2021; Ankle syndesmotic injury: tightrope vs screw fixation, a clinical academic survey. Ann Med Surg (Lond). 69:102680. doi: 10.1016/j.amsu.2021.102680. DOI: 10.1016/j.amsu.2021.102680. PMID: 34429950. PMCID: PMC8371209.
Article13. Van Heest TJ, Lafferty PM. 2014; Injuries to the ankle syndesmosis. J Bone Joint Surg Am. 96:603–13. doi: 10.2106/JBJS.M.00094. DOI: 10.2106/JBJS.M.00094. PMID: 24695928.
Article14. Klitzman R, Zhao H, Zhang LQ, Strohmeyer G, Vora A. 2010; Suture-button versus screw fixation of the syndesmosis: a biomechanical analysis. Foot Ankle Int. 31:69–75. doi: 10.3113/FAI.2010.0069. DOI: 10.3113/FAI.2010.0069. PMID: 20067726.
Article15. LaMothe JM, Baxter JR, Murphy C, Gilbert S, DeSandis B, Drakos MC. 2016; Three-dimensional analysis of fibular motion after fixation of syndesmotic injuries with a screw or suture-button construct. Foot Ankle Int. 37:1350–6. doi: 10.1177/1071100716666865. DOI: 10.1177/1071100716666865. PMID: 27654046.
Article16. Schepers T, van Zuuren WJ, van den Bekerom MP, Vogels LM, van Lieshout EM. 2012; The management of acute distal tibio-fibular syndesmotic injuries: results of a nationwide survey. Injury. 43:1718–23. doi: 10.1016/j.injury.2012.06.015. DOI: 10.1016/j.injury.2012.06.015. PMID: 22795845.
Article17. Moore JA Jr, Shank JR, Morgan SJ, Smith WR. 2006; Syndesmosis fixation: a comparison of three and four cortices of screw fixation without hardware removal. Foot Ankle Int. 27:567–72. doi: 10.1177/107110070602700801. DOI: 10.1177/107110070602700801. PMID: 16919207.
Article18. Olerud C. 1985; The effect of the syndesmotic screw on the extension capacity of the ankle joint. Arch Orthop Trauma Surg (1978). 104:299–302. doi: 10.1007/BF00435946. DOI: 10.1007/BF00435946. PMID: 4091635.
Article19. Pallis MP, Pressman DN, Heida K, Nicholson T, Ishikawa S. 2018; Effect of ankle position on tibiotalar motion with screw fixation of the distal tibiofibular syndesmosis in a fracture model. Foot Ankle Int. 39:746–50. doi: 10.1177/1071100718759966. DOI: 10.1177/1071100718759966. PMID: 29600720.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current Trends in the Treatment of Diabetic Foot: Analysis of the Korean Foot and Ankle Society (KFAS) Member Survey
- Current Trends in the Treatment of Diabetic Foot: Analysis of the Korean Foot and Ankle Society (KFAS) Member Survey
- Isolated Syndesmotic Injury
- Current Trends in the Treatment of Acute Achilles Tendon Rupture: Analysis of the Korean Foot and Ankle Society (KFAS) Member Survey
- Current Trends in the Treatment of Ankle Arthritis: Analysis of the Korean Foot and Ankle Society (KFAS) Member Survey
