Paraesophageal Anthracofibrosis Mimicking Metastatic Lymphadenopathy in Papillary Thyroid Cancer: a Case Report
- Affiliations
-
- 1Departments of Otorhinolaryngology-Head and Neck Surgery, Chonnam National University Medical School and Hwasun Hospital, Hwasun, Korea
- 2Departments of Pathology , Chonnam National University Medical School and Hwasun Hospital, Hwasun, Korea
- KMID: 2530126
- DOI: http://doi.org/10.11106/ijt.2022.15.1.49
Abstract
- Anthracofibrosis is luminal narrowing with a black anthracotic pigmentation on the bronchial mucosa. Extrapulmonary anthracofibrosis is very rare in head and neck region, and anthracofibrosis associated with adhesion to adjacent tissue can be misdiagnosed to malignancy. We report a rare case of a paraesophageal anthracofibrosis in a patient with advanced papillary thyroid cancer. The paraesophageal anthracofibrosis presented as a black colored hard mass with severe adhesion to the recurrent laryngeal nerve (RLN) during thyroid surgery, suspecting metastatic lymphadenopathy. With intraoperative frozen biopsy, unnecessary aggressive surgery with the injury of RLN can be avoided. Permanent histopathological examination of the mass revealed anthracofibrosis with strong positivity on Masson’s trichrome staining. This case highlights that anthracofibrosis should be included in differential diagnosis of paraesophageal masses, and frozen sectional biopsy can help in decision making during surgery. In addition, collagen might be involved in the adhesion of the anthracotic mass to the surrounding tissues.
Figure
-
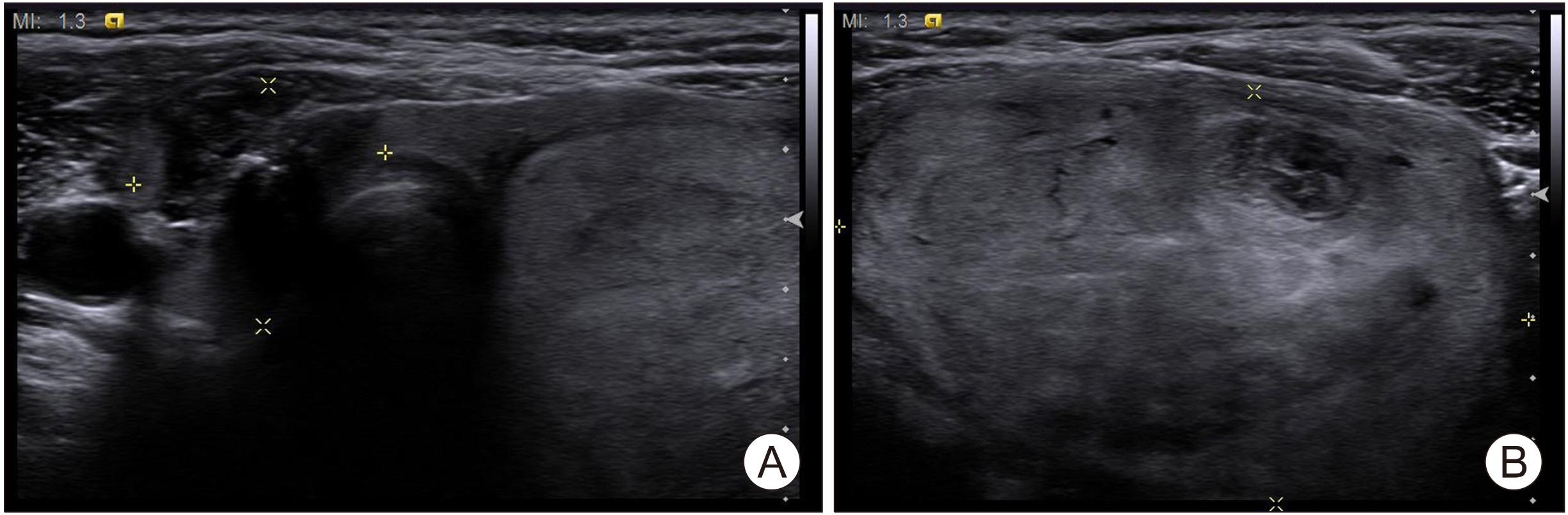
Fig. 1 Thyroid ultrasonography showing a 1.8× 1.7×2.2-cm hypoechoic, ill-defined mass with microcalcification and extrathyroidal invasion in the right thyroid gland (A) and a 5.7× 3.4×5.9-cm mixed-echoic mass in the left thyroid gland (B).
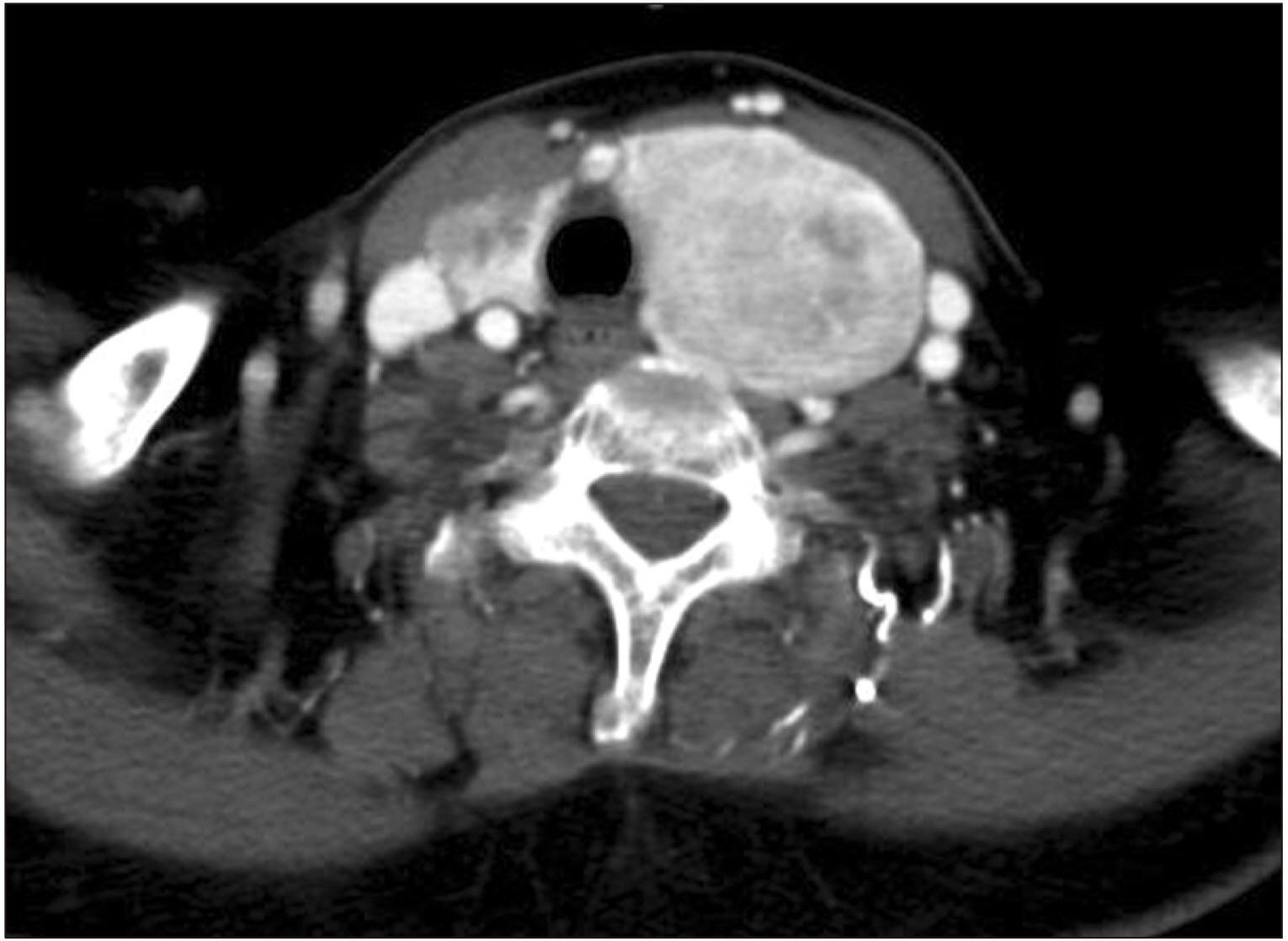
Fig. 2 Neck computed tomography with enhancement showing a 2.2×1.8×1.4-cm irregular subtle enhancing low attenuated nodule with calcification and extrathyroidal extension in the right thyroid gland and a 7×4.5×5-cm heterogeneously enhancing mass in the left thyroid gland.
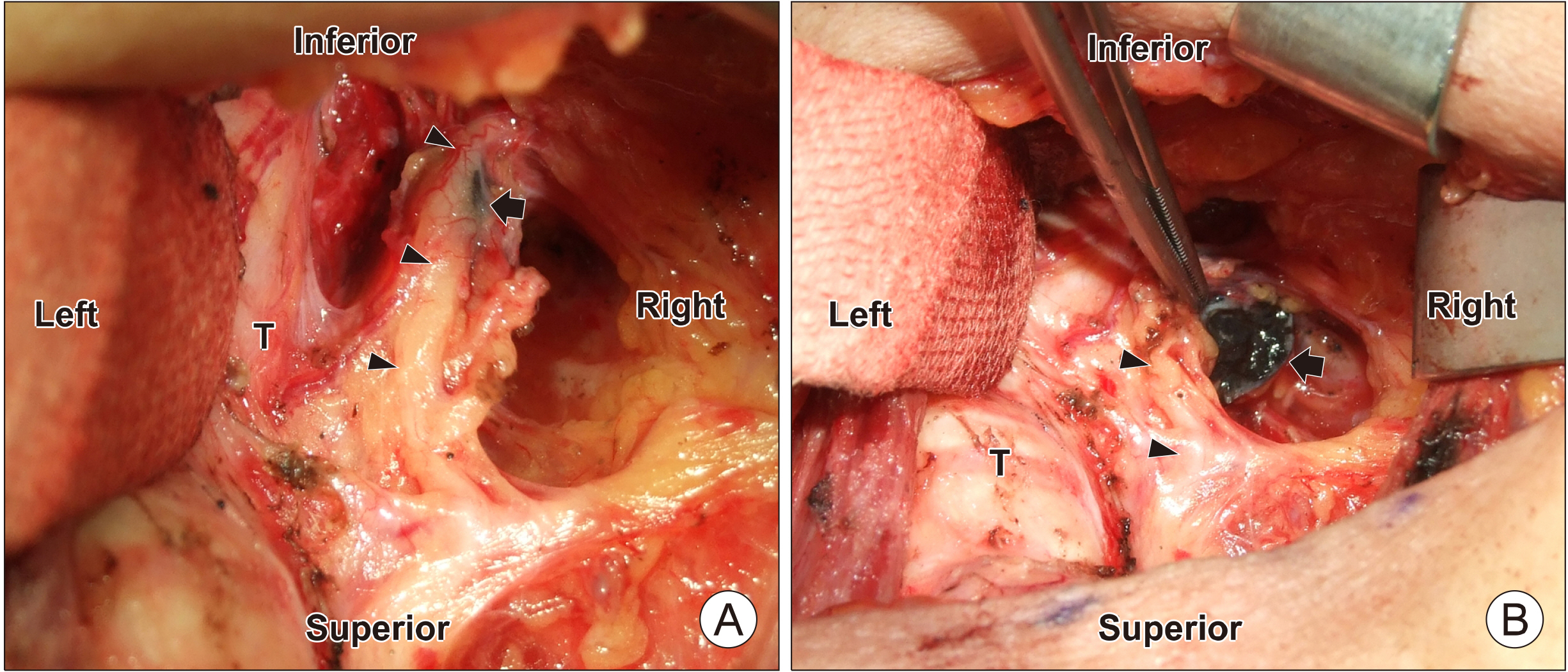
Fig. 3 Operative findings after thyroidectomy shows a 1.5-cm black colored, right paraesophageal mass (black arrow), suspected as metastatic lymphadenopathy, under the right recurrent laryngeal nerve (black arrowheads) (A). The cut surface of the mass (black arrow) obtained for intraoperative frozen sectional biopsy was as black as coal. Black arrowheads indicated the right recurrent laryngeal nerve (B). T: trachea
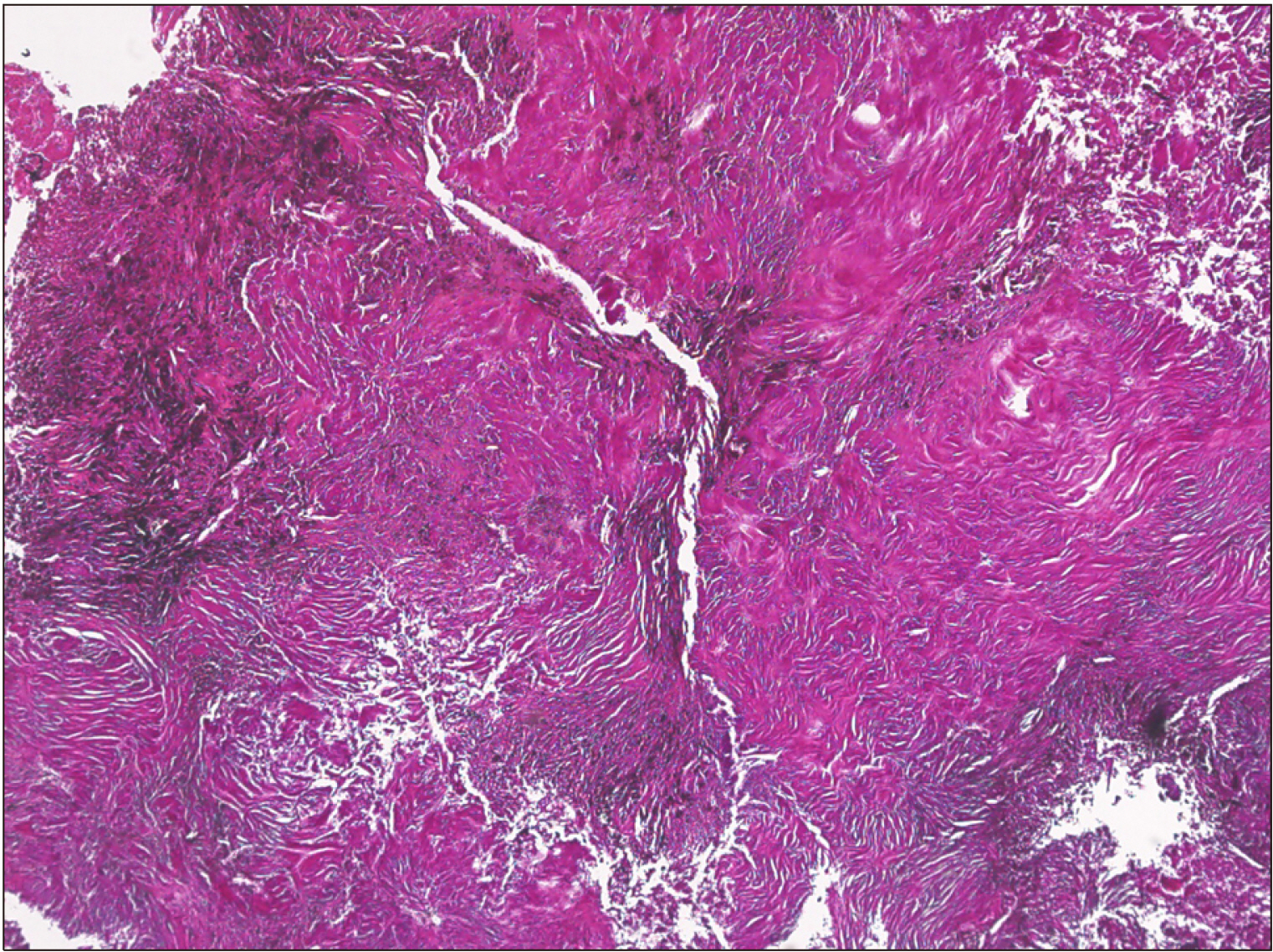
Fig. 4 Histopathological examination of the paraesophageal mass revealed anthracotic pigment deposition and dense fibrotic changes (Hematoxylin and Eosin [H&E] stain, ×40).

Fig. 5 Histopathological findings of Masson’s Trichrome staining (MT, ×200) in 4 cases with anthracosis. (A) This case and another case with a paratracheal mass had severe adhesion to adjacent tissues. A prominent increase in blue collagen fibers were seen on MT staining. (B) Two other cases of cervical anthracosis had no adhesion to adjacent tissues. These cases showed negative on MT staining (H&E stain, ×100).
Reference
-
References
1. Mirsadraee M, Asna-Ashari A, Attaran D, Naghibi S, Mirsadraee S. 2013; Bronchial anthracosis: a new diagnosis for benign mass lesions of the lung. Tanaffos. 12(4):10–8. PMID: 25191478. PMCID: PMC4153268.2. Chung MP, Lee KS, Han J, Kim H, Rhee CH, Han YC, et al. 1998; Bronchial stenosis due to anthracofibrosis. Chest. 113(2):344–50. DOI: 10.1378/chest.113.2.344. PMID: 9498950.
Article3. Bilici A, Erdem T, Boysan SN, Acbay O, Oz B, Besirli K, et al. 2003; A case of anthracosis presenting with mediastinal lymph nodes mimicking tuberculous lymphadenitis or malignancy. Eur J Intern Med. 14(7):444–6. DOI: 10.1016/j.ejim.2003.09.001. PMID: 14614980.
Article4. Onitilo AA, Engel JM, Tanimu SB, Nguyen TC. 2010; Anthracosis and large mediastinal mass in a patient with healed pulmonary tuberculosis. Clin Med Res. 8(2):99–103. DOI: 10.3121/cmr.2010.876. PMID: 20660934. PMCID: PMC2910103.
Article5. Yoon TM, Lee DH, Lee JK, Lim SC. 2012; A case of anthracofibrosis presenting with paratracheal mass compressing trachea. Otolaryngol Head Neck Surg. 147(3):592–3. DOI: 10.1177/0194599812441916. PMID: 22434100.
Article6. Choi SN, Kim TH, Kim HJ, Ha CY, Min HJ, Jung WT, et al. 2010; Esophageal anthracosis complicated by mediastinal tuberculous lymphadenitis presenting as submucosal tumor. Gastrointest Endosc. 72(3):651–3. DOI: 10.1016/j.gie.2009.12.019. PMID: 20417505.
Article7. Cserni G. 1998; Misidentification of an axillary sentinel lymph node due to anthracosis. Eur J Surg Oncol. 24(3):168. DOI: 10.1016/S0748-7983(98)92844-X. PMID: 9630853.
Article8. Kim JY, Park JS, Kang MJ, Yu CG, Kim YH, Han SG, et al. 1996; Endobronchial anthracofibrosis is causally associated with tuberculosis. Korean J Intern Med. 51(3):351–7. DOI: 10.22246/jikm.2021.42.3.351.9. Garvey W. 1984; Modified elastic tissue-Masson trichrome stain. Stain Technol. 59(4):213–6. DOI: 10.3109/10520298409113858. PMID: 6208643.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple Cervical Schwannomas Mimicking Metastatic Lymph Nodes from Papillary Thyroid Cancer
- Benign Schwannoma Mimicking Metastatic Lesion on F-18 FDG PET/CT in Differentiated Thyroid Cancer
- Concurrent Primary Carcinoma and Metastatic Lesions of the Thyroid
- Metastatic Lung Nodule of Thyroid Papillary Carcinoma, Mimicking Primary Lung Cancer
- Kikuchi-Fujimoto Disease Coexistent with Papillary Thyroid Carcinoma in a Single Lymph Node
