Drilling off the Petrosal Apex and Opening the Upper Wall of Meckel’s Cave Are the Key Elements of Good Outcomes in the Treatment of Trigeminal Neuralgia Secondary to Petrous Apex Meningioma
- Affiliations
-
- 1Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, China
- 2Department of Neurosurgery, Fuzhou First People's Hospital, Fifth Affiliated Hospital of Nanchang University, Nanchang, China
- KMID: 2529593
- DOI: http://doi.org/10.3340/jkns.2021.0060
Abstract
Objective
: The surgical management of trigeminal neuralgia (TN) caused by petrous apex meningioma (PAM) is still a challenge because of the lesion’s deep location and the surrounding complex structures. The authors describe the intradural anterior transpetrosal approach (ATPA) and its effect on the treatment of TN secondary to PAM.
Methods
: A retrospective analysis of 15 patients with TN secondary to PAM who underwent surgery via the intradural ATPA was conducted. The key techniques, which included drilling off the petrosal apex (PA) and opening the upper wall of Meckel’s cave (MC), are described in detail.
Results
: Total removal of the tumor and complete pain relief (Barrow Neurological Institute I) were achieved in all 15 patients without significant morbidity. Five patients developed new facial numbness postoperatively, which disappeared within three months after surgery. The postoperative magnetic resonance imaging showed temporal lobe swelling in three patients, but no clinical symptoms. One patient had cerebrospinal fluid leakage and was managed with bed rest and temporary lumbar drainage. One patient had an intracranial infection and was treated with antibiotics. By the last follow up, no patients had pain relapse or/and tumor recurrence. It is worth noting that the vascular compression at the root of the trigeminal nerve was found in one patient during the operation.
Conclusion
: Our experience suggests that drilling off the PA and opening the upper wall of the MC are key elements for a good outcome of the treatment of TN secondary to PAM. The intradural ATPA has the advantages for both tumor resection and pain relief.
Keyword
Figure
-

Fig. 1. Magnetic resonance imaging (MRI) images of petrous apex meningioma. A and B : Preoperative contrast MRI images. There is a tumor significant enhancement (white arrow) located at right petrous apex extended to MC and upper clivus. C and D : Postoperative contrast MRI images. The tumor was gross totally removed (white arrow).
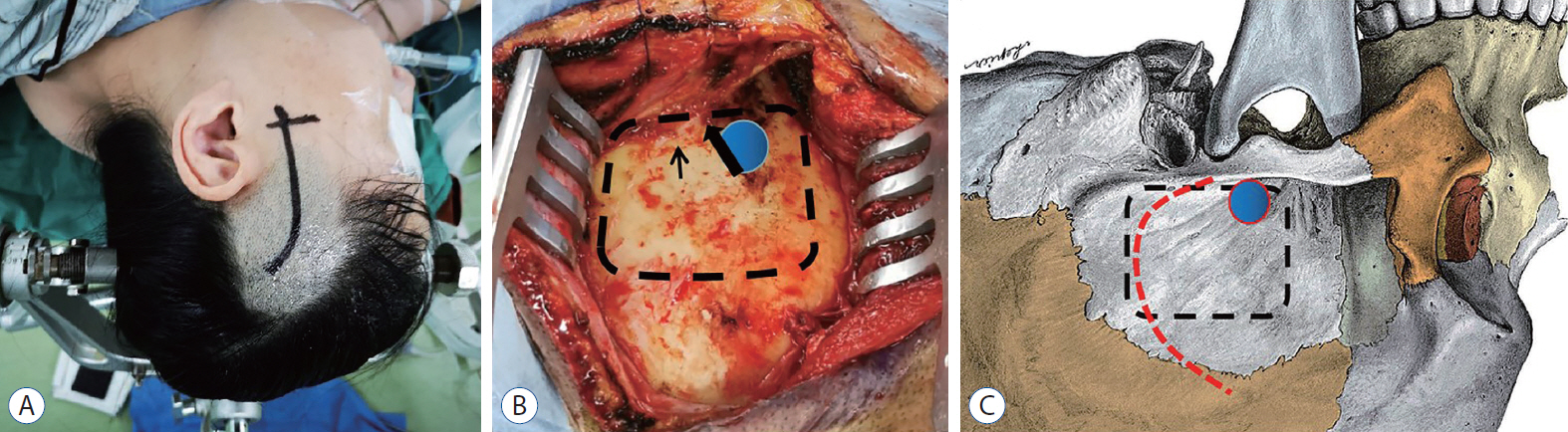
Fig. 2. Position, skin incision and craniotomy of patient. A : The patient was placed in a lateral decubitus position. The head was fixed in a three-point Mayfield head holder. The curvilinear skin incision was used. B : Exposure of temporal bone. Burr hole (blue circle) was drilled above root of zygomatic arch (black thick arrow) and bone flap (black dashed line) was removed and the basement is at the level of the superior crest of the external auditory canal (black thin arrow). C : Sketch map showed burr hole (blue circle), bone flap (black dashed line) and incision of temporalis fascia and muscle (red dashed line).
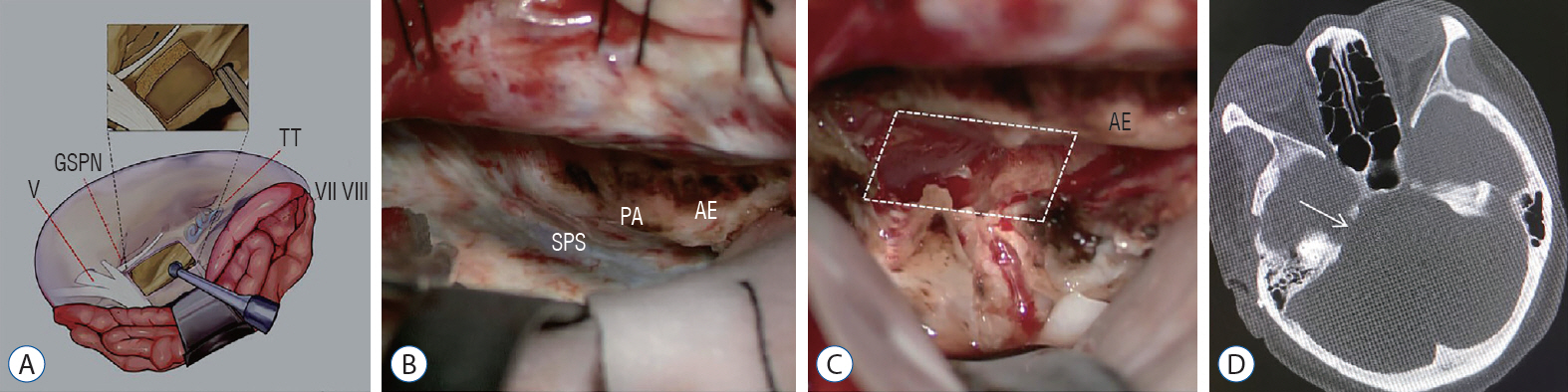
Fig. 3. Removing bone of PA. A : Illustration showing the drilling extent of petrous apex bone. The trigeminal impression, the posterior edge of petrous ridge and AE were used as landmarks. B : PA, SPS, and AE was exposed by retracting temporal lobe in operation. C : Bone of PA (Kawase triangle) was drilled out (white dashed line) in operation. D : The postoperative thin-slice computed tomography shows the drilling range of petrous apex bone (white arrow). V : cranial nerve V, GSPN : great superficial petrous nerve, TT : tegmen tympani, VII : cranial nerve VII, VIII : VIII cranial nerve, SPS : superior petrosal sinus, PA : petrous apex, AE : arcuate eminence.
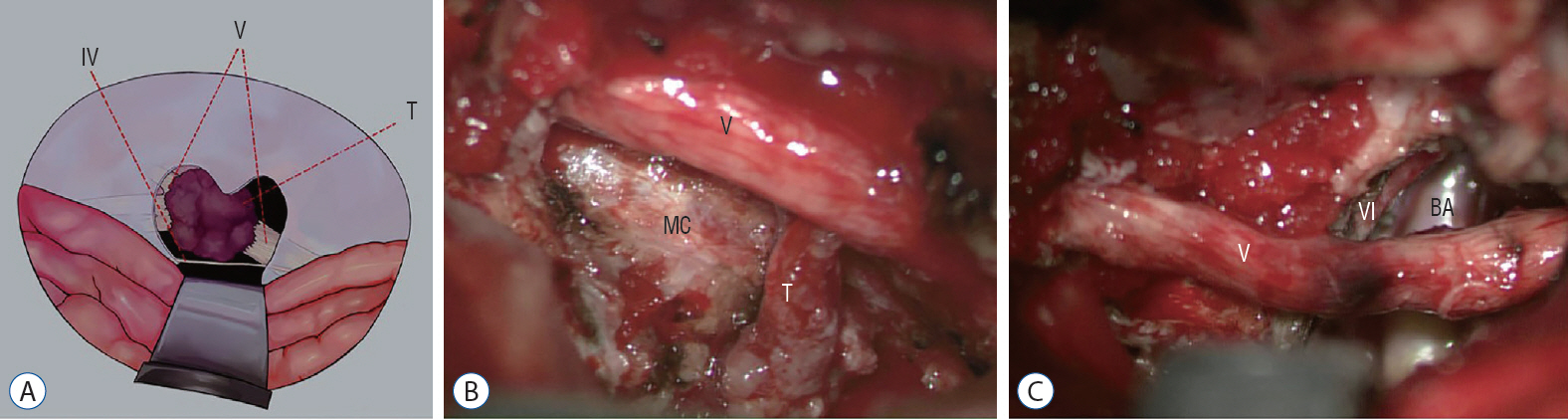
Fig. 4. Opening the upper wall of the Meckel’s cave (MC) and removing tumor totally. A : Illustration showing the removing extent of the up wall of MC and the tentorium. B : Opening the Meckel Cave and removing the tumor in it during the operation. C : After removing tumor totally, trigeminal nerve, abducens nerve and BA were exposed. IV : cranial nerve, V : cranial nerve V, T : tumor, BA : basilar artery.
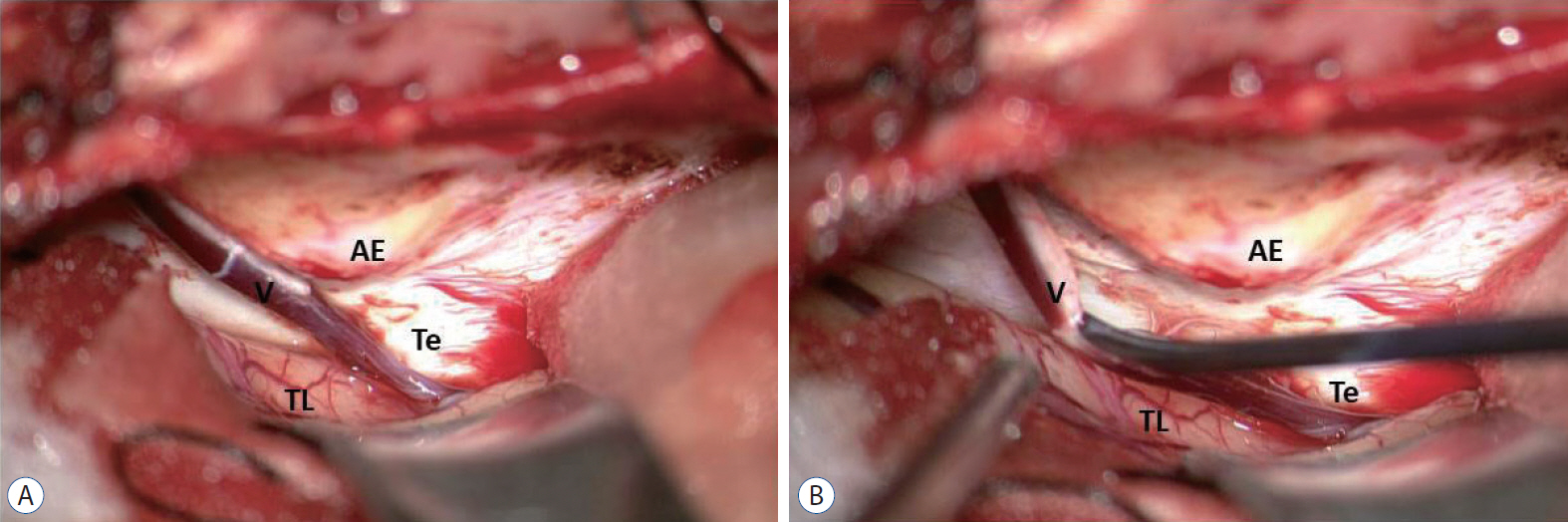
Fig. 5. The management of temporal drainage vein. A : The temporal drainage vein passed through the dura mater of skull base and drain posteriorly. B : The temporal drainage vein was dissected from dura mater of skull base and pull to temporal lobe. AE : arcuate eminence, Te : tentorium, TL : temporal lobe, V : vein.

Fig. 6. The management of air cells of PA after removing the tumor totally. A : The air cells may be opened after drilling off PA. B : The PA was sealed by a piece of muscle with fibrin glue. AE : arcuate eminence, M : muscle, PA : petrous apex.
Reference
-
References
1. Almefty R, Dunn IF, Pravdenkova S, Abolfotoh M, Al-Mefty O. True petroclival meningiomas: results of surgical management. J Neurosurg. 120:40–51. 2014.
Article2. Barker FG 2nd, Jannetta PJ, Babu RP, Pomonis S, Bissonette DJ, Jho HD. Long-term outcome after operation for trigeminal neuralgia in patients with posterior fossa tumors. J Neurosurg. 84:818–825. 1996.
Article3. Berti A, Granville M, Wu X, Huang D, Schwade JG, Jacobson RE. Delayed development of trigeminal neuralgia after radiosurgical treatment of a tentorial meningioma. Cureus. 9:e1628. 2017.
Article4. Bir SC, Maiti TK, Bollam P, Nanda A. Management of recurrent trigeminal neuralgia associated with petroclival meningioma. J Neurol Surg B Skull Base. 77:47–53. 2016.
Article5. Black PM. Hormones, radiosurgery and virtual reality: new aspects of meningioma management. Can J Neurol Sci. 24:302–306. 1997.
Article6. Bullitt E, Tew JM, Boyd J. Intracranial tumors in patients with facial pain. J Neurosurg. 64:865–871. 1986.
Article7. Chen LF, Yu XG, Bu B, Xu BN, Zhou DB. The retrosigmoid approach to petroclival meningioma surgery. J Clin Neurosci. 18:1656–1661. 2011.
Article8. Cho CW, Al-Mefty O. Combined petrosal approach to petroclival meningiomas. Neurosurgery. 51:708–716. discussion 716-718. 2002.
Article9. Cui H, Zhou CF, Bao YH, Wang MS, Wang Y. Extended suboccipital retrosigmoid surgical approach is effective for resection of petrous apex meningioma. J Craniofac Surg. 27:e429–e433. 2016.
Article10. de Divitiis O, Elefante A, de Divitiis E. Which strategy for petroclival tumors? World Neurosurg. 86:33–35. 2016.
Article11. Diaz Day J. The middle fossa approach and extended middle fossa approach: technique and operative nuances. Neurosurgery. 70(2 Suppl Operative):192–201. 2012.12. Dumot C, Brinzeu A, Berthiller J, Sindou M. Trigeminal neuralgia due to venous neurovascular conflicts: outcome after microvascular decompression in a series of 55 consecutive patients. Acta Neurochir (Wien). 159:237–249. 2017.
Article13. Gerganov VM, Giordano M, Elolf E, Osamah A, Amir S, Madjid S. Operative management of patients with radiosurgery-related trigeminal neuralgia: analysis of the surgical morbidity and pain outcome. Clin Neurol Neurosurg. 122:23–28. 2014.
Article14. Goel A. Extended lateral subtemporal approach for petroclival meningiomas: report of experience with 24 cases. Br J Neurosurg. 13:270–275. 1999.
Article15. Hegazy A, Alfiki A, Adel MF, Alsawy MF, Al-Dash MF, Zein M, et al. Role of surgery for small petrous apex meningiomas causing refractory trigeminal neuropathy in the minimally invasive era. Neurol India. 64:973–979. 2016.
Article16. Ichimura S, Hori S, Hecht N, Czabanka M, Vajkoczy P. Intradural anterior transpetrosal approach. Neurosurg Rev. 39:625–631. 2016.
Article17. Kai M, Yongjie L. Clinical features and surgical management of cerebellopontine angle cholesteatoma that presented as trigeminal neuralgia. World Neurosurg. 115:e7–e12. 2018.
Article18. Kano H, Awan NR, Flannery TJ, Iyer A, Flickinger JC, Lunsford LD, et al. Stereotactic radiosurgery for patients with trigeminal neuralgia associated with petroclival meningiomas. Stereotact Funct Neurosurg. 89:17–24. 2011.
Article19. Karam SD, Tai A, Wooster M, Rashid A, Chen R, Baig N, et al. Trigeminal neuralgia treatment outcomes following Gamma Knife radiosurgery with a minimum 3-year follow-up. J Radiat Oncol. 3:125–130. 2014.
Article20. Kawase T, Shiobara R, Ohira T, Toya S. Developmental patterns and characteristic symptoms of petroclival meningiomas. Neurol Med Chir (Tokyo). 36:1–6. 1996.
Article21. Kawase T, Shiobara R, Toya S. Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas: surgical method and results in 10 patients. Neurosurgery. 28:869–875. discussion 875-876. 1991.
Article22. Kouzounias K, Lind G, Schechtmann G, Winter J, Linderoth B. Comparison of percutaneous balloon compression and glycerol rhizotomy for the treatment of trigeminal neuralgia. J Neurosurg. 113:486–492. 2010.
Article23. Liao CH, Wang JT, Lin CF, Chen SC, Lin CJ, Hsu SPC, et al. Pretemporal trans-Meckel's cave transtentorial approach for large petroclival meningiomas. Neurosurg Focus. 44:E10. 2018.
Article24. Little AS, Jittapiromsak P, Crawford NR, Deshmukh P, Preul MC, Spetzler RF, et al. Quantitative analysis of exposure of staged orbitozygomatic and retrosigmoid craniotomies for lesions of the clivus with supratentorial extension. Neurosurgery. 62(5 Suppl 2):ONS318–ONS323. discussion ONS323-ONS324. 2018.
Article25. Martínez-Pérez R, Silveira-Bertazzo G, Rangel GG, Albiña P, Hardesty D, Carrau RL, et al. The historical perspective in approaches to the spheno-petro-clival meningiomas. Neurosurg Rev. 44:51–60. 2021.
Article26. Mathiesen T, Gerlich A, Kihlström L, Svensson M, Bagger-Sjöbäck D. Effects of using combined transpetrosal surgical approaches to treat petroclival meningiomas. Neurosurgery. 60:982–991. discussion 991-992. 2007.
Article27. Mureb MC, Dastazirgada Y, Benjamin C, Golfinos JG, Kondziolka D. Simultaneous treatment of petroclival meningiomas and the trigeminal nerve with gamma knife radiosurgery for tumor-related trigeminal neuralgia. World Neurosurg. 139:242–244. 2020.
Article28. Natarajan SK, Sekhar LN, Schessel D, Morita A. Petroclival meningiomas: multimodality treatment and outcomes at long-term follow-up. Neurosurgery. 60:965–979. discussion 979-981. 2007.
Article29. Nicolato A, Ferraresi P, Foroni R, Pasqualin A, Piovan E, Severi F, et al. Gamma knife radiosurgery in skull base meningiomas. Preliminary experience with 50 cases. Stereotact Funct Neurosurg 66 Suppl. 1:112–120. 1996.30. Obermann M. Treatment options in trigeminal neuralgia. Ther Adv Neurol Disord. 3:107–115. 2010.
Article31. Pollock BE, Iuliano BA, Foote RL, Gorman DA. Stereotactic radiosurgery for tumor-related trigeminal pain. Neurosurgery. 46:576–582. discussion 582-583. 2000.
Article32. Ramina R, Neto MC, Fernandes YB, Silva EB, Mattei TA, Aguiar PH. Surgical removal of small petroclival meningiomas. Acta Neurochir (Wien). 150:431–438. discussion 438-439. 2008.
Article33. Rolston JD, Han SJ, Lau CY, Berger MS, Parsa AT. Frequency and predictors of complications in neurological surgery: national trends from 2006 to 2011. J Neurosurg. 120:736–745. 2014.
Article34. Samii M, Carvalho GA, Tatagiba M, Matthies C. Surgical management of meningiomas originating in Meckel's cave. Neurosurgery. 41:767–774. discussion 774-775. 1997.
Article35. Samii M, Rosahl SK, Tatagiba MS. Microsurgical removal of a petrous apex meningioma after stereotactic radiation: technical case report. Neurosurgery. 49:216–219. discussion 219-220. 2001.
Article36. Samii M, Tatagiba M, Carvalho GA. Resection of large petroclival meningiomas by the simple retrosigmoid route. J Clin Neurosci. 6:27–30. 1999.
Article37. Samii M, Tatagiba M, Carvalho GA. Retrosigmoid intradural suprameatal approach to Meckel's cave and the middle fossa: surgical technique and outcome. J Neurosurg. 92:235–241. 2000.
Article38. Seifert V, Raabe A, Zimmermann M. Conservative (labyrinth-preserving) transpetrosal approach to the clivus and petroclival region--indications, complications, results and lessons learned. Acta Neurochir (Wien). 145:631–642. discussion 642. 2003.
Article39. Shulev Y, Trashin A, Gordienko K. Secondary trigeminal neuralgia in cerebellopontine angle tumors. Skull Base. 21:287–294. 2011.
Article40. Squire SE, Chan MD, Furr RM, Lowell DA, Tatter SB, Ellis TL, et al. Gamma knife radiosurgery in the treatment of tumor-related facial pain. Stereotact Funct Neurosurg. 90:145–150. 2012.
Article41. Steiger HJ, Hänggi D, Stummer W, Winkler PA. Custom-tailored transdural anterior transpetrosal approach to ventral pons and retroclival regions. J Neurosurg. 104:38–46. 2006.
Article42. Tuleasca C, Régis J, Sahgal A, De Salles A, Hayashi M, Ma L, et al. Stereotactic radiosurgery for trigeminal neuralgia: a systematic review. J Neurosurg. 130:733–757. 2018.
Article43. Xiao X, Zhang L, Wu Z, Zhang J, Jia G, Tang J, et al. Surgical resection of large and giant petroclival meningiomas via a modified anterior transpetrous approach. Neurosurg Rev. 36:587–593. discussion 593-594. 2013.
Article44. Yamakami I, Higuchi Y, Horiguchi K, Saeki N. Treatment policy for petroclival meningioma based on tumor size: aiming radical removal in small tumors for obtaining cure without morbidity. Neurosurg Rev. 34:327–334. discussion 334-335. 2011.
Article45. Yang J, Liu YH, Ma SC, Wei L, Lin RS, Qi JF, et al. Subtemporal transtentorial petrosalapex approach for giant petroclival meningiomas: analyzation and evaluation of the clinical application. J Neurol Surg B Skull Base. 73:54–63. 2012.
Article46. Yang J, Ma SC, Fang T, Qi JF, Hu YS, Yu CJ. Subtemporal transpetrosal apex approach: study on its use in large and giant petroclival meningiomas. Chin Med J (Engl). 124:49–55. 2011.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Petrous Apex Cephalocele: Report of Two Cases and Review of the Literature
- Suboccipital Suprameatal Approach for Petrosal Meningiomas Extended into Meckel's Cave
- Meckel’s cave compression with Teflon for the treatment of idiopathic trigeminal neuralgia: its possibility as a modified surgical technique
- New Technique for Surgery of Petrous Apex Cholesterol Granuloma
- Surgical Anatomy for the Infracochlear Approach to the Petrous Apex
