Intraoperative monitoring of cortico-cortical evoked potentials of the frontal aslant tract in a patient with oligodendroglioma
- Affiliations
-
- 1Department of Neurology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Department of Neurosurgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2529503
- DOI: http://doi.org/10.14253/acn.2022.24.1.21
Abstract
- The newly identified frontal aslant tract (FAT) that connects the posterior Broca’s area to the supplementary motor area is known to be involved in speech and language functions. We successfully intraoperatively monitored FAT using cortico-cortical evoked potentials generated by single-pulse electrical cortical stimulation in a patient with oligodendroglioma.
Figure
-
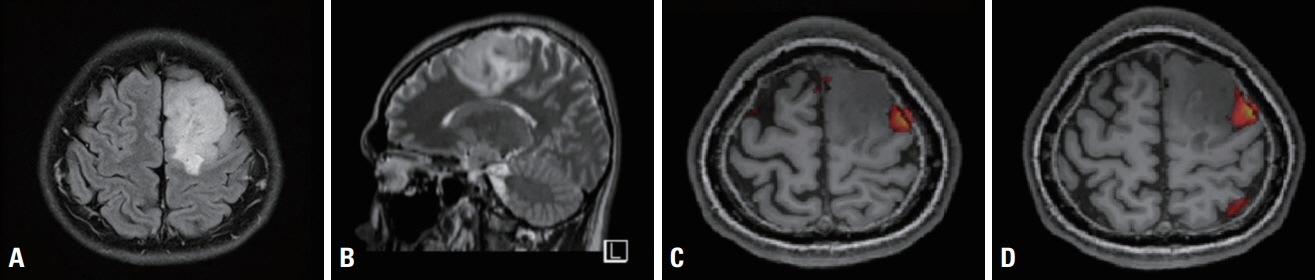
Fig. 1. Brain magnetic resonance imaging (MRI) and functional MRI of the patient. Fluid attenuated inversion recovery axial (A) and T2-weighted sagittal (B) MRI revealed a mass in the left supplementary motor area, suggestive of low-grade glioma. Functional MRI (C, D) showed increased blood-oxygen-level-dependent signals in the left frontal cortex adjacent to the mass during verbal language tasks.
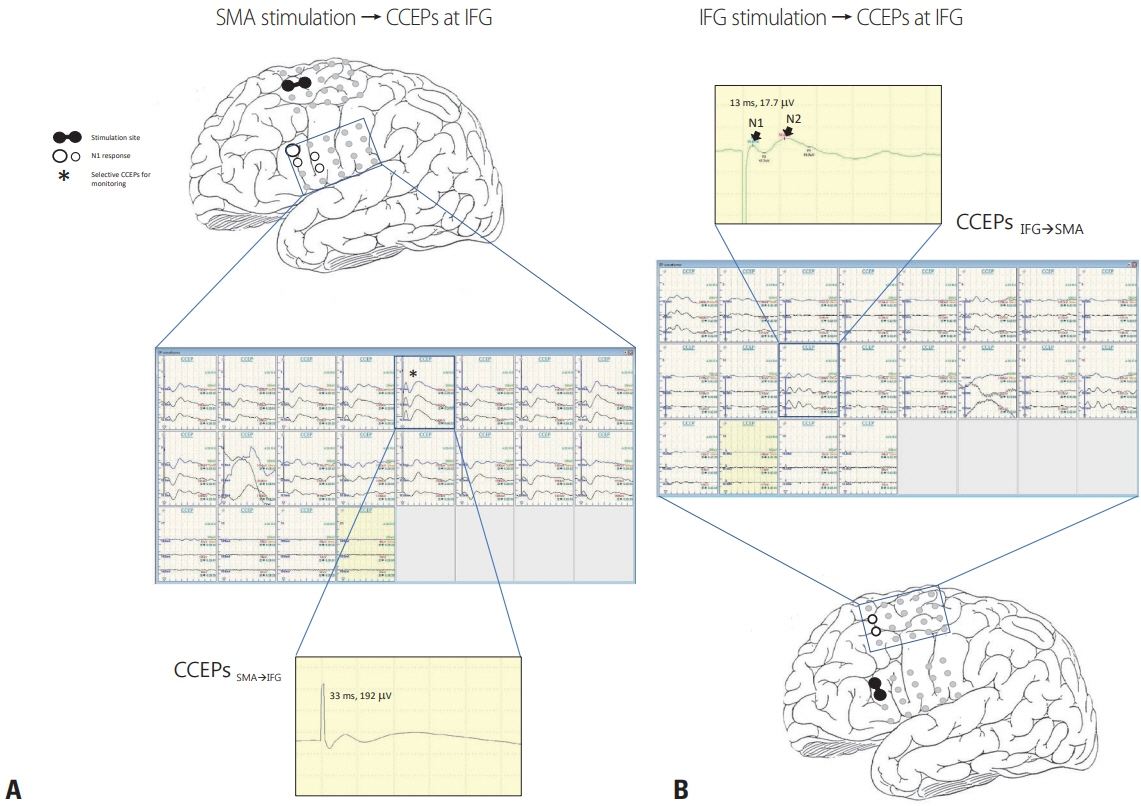
Fig. 2. Schema of intraoperative CCEPs. (A) Single-pulse electrical stimulation of the SMA (black circle pair) produced CCEPs in inferior frontal gyrus (CCEPSMA→IFG). The latencies and amplitudes of the maximal N1 response (white circles with black rim) in CCEPSMA→IFG were 33 ms and 192 mV. (B) By stimulating corresponding pairs of electrodes on the IFG, the optimal CCEP pathways could be confirmed. The latencies and amplitudes of the maximal N1 response of the main CCEPIFG→SMA were 13 ms and 17.5 mV, which had a shorter latency and were smaller than for CCEPSMA→IFG. CCEPs generally show an early sharp negative potential (N1: peak latency 10–50 ms) and a sequential slow negative potential (N2: peak latency 50–300 ms).6 SMA, supplementary motor area; CCEPs, cortico-cortical evoked potentials; IFG, inferior frontal gyrus.

Fig. 3. Serial cortico-cortical evoked potentials (CCEPs) during tumor removal. CCEP monitoring revealed no abnormal N1 response of CCEPSMA→IFG until the surgery was completed. SMA, supplementary motor area; IFG, inferior frontal gyrus.
Reference
-
1. Kim SM, Kim SH, Seo DW, Lee KW. Intraoperative neurophysiologic monitoring: basic principles and recent update. J Korean Med Sci. 2013; 28:1261–1269.
Article2. Matsumoto R, Nair DR, LaPresto E, Najm I, Bingaman W, Shibasaki H, et al. Functional connectivity in the human language system: a cortico-cortical evoked potential study. Brain. 2004; 127:2316–2330.
Article3. Fujii M, Maesawa S, Motomura K, Futamura M, Hayashi Y, Koba I, et al. Intraoperative subcortical mapping of a language-associated deep frontal tract connecting the superior frontal gyrus to Broca’s area in the dominant hemisphere of patients with glioma. J Neurosurg. 2015; 122:1390–1396.
Article4. Ookawa S, Enatsu R, Kanno A, Ochi S, Akiyama Y, Kobayashi T, et al. Frontal fibers connecting the superior frontal gyrus to Broca area: a corticocortical evoked potential study. World Neurosurg. 2017; 107:239–248.
Article5. La Corte E, Eldahaby D, Greco E, Aquino D, Bertolini G, Levi V, et al. The frontal aslant tract: a systematic review for neurosurgical applications. Front Neurol. 2021; 12:641586.
Article6. Yamao Y, Matsumoto R, Kikuchi T, Yoshida K, Kunieda T, Miyamoto S. Intraoperative brain mapping by cortico-cortical evoked potential. Front Hum Neurosci. 2021; 15:635453.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative Language Area Mapping: Cortico-Cortical Evoked Potential
- Intraoperative monitoring of flash visual evoked potential under general anesthesia
- Intraoperative Neurophysiologic Monitoring: Basic Principles and Recent Update
- Intraoperative Monitoring for Tethered Cord Syndrome Using Somatosensory Evoked Potential and Motor Evoked Potential: Report of three cases
- Monitoring of Somatosensory Evoked Potentials During Intracranial Aneurysm Surgery
