Reconstruction of the sciatic nerve using bilateral vascularized sural nerve grafts: a case report
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Jeonbuk National University Medical School, Jeonju, Korea
- KMID: 2526657
- DOI: http://doi.org/10.12790/ahm.21.0125
Abstract
- An injury of a peripheral nerve may require reconstruction for motor and sensory function recovery. However, if the nerve defect is long, especially in the lower extremities, reconstruction with successful functional recovery has proven to be difficult. We documented a case of bilateral vascularized sural nerve graft repair of a large and long sciatic nerve defect following malignant tumor resection on the posterior thigh. Although we were unable to achieve satisfactory outcomes in motor function recovery, we did achieve some degree of sensory function recovery.
Figure
-
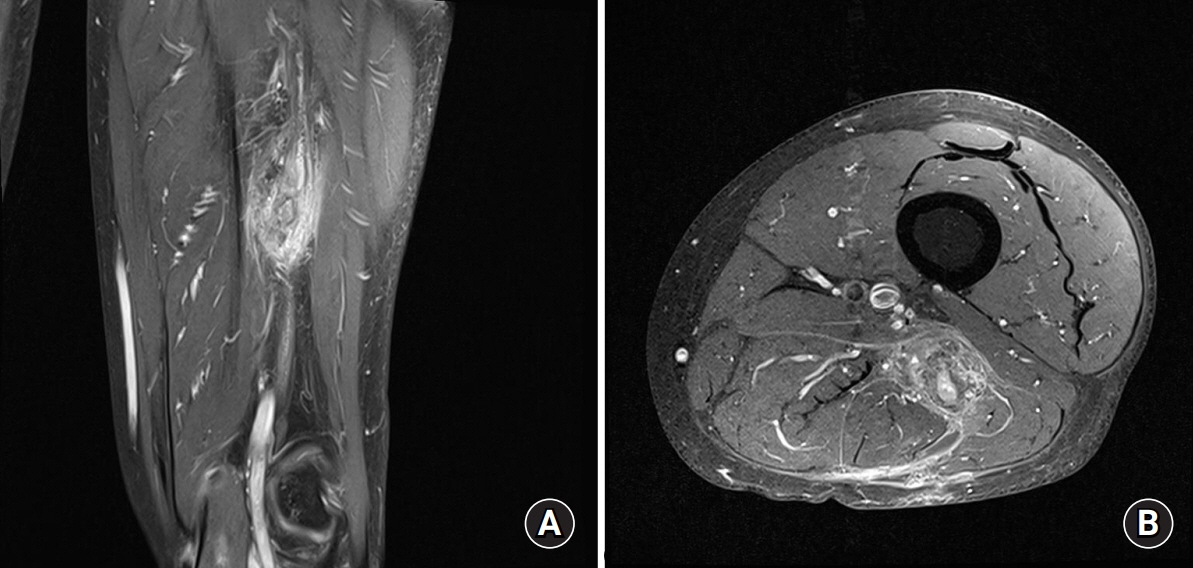
Fig. 1. Magnetic resonance images of the left posterior thigh. (A) Sagittal view. (B) Axial view. In front of the hamstring muscle, a mass measuring about 1.0×6.0×2.0 cm attached to the sciatic nerve is shown.

Fig. 2. The tumor mass was located on the sciatic nerve and involved the surrounding muscles.

Fig. 3. After wide excision of the tumor mass including the sciatic nerve and surrounding tissues, an 8-cm sciatic nerve defect is shown around 4 cm above the bifurcation site.

Fig. 4. The sural nerve, including the lesser saphenous vein and the fascia, was elevated and harvested en bloc to form a vascularized flap from both lower legs. (A) Right lower leg. (B) Left lower leg. (C) Vascularized sural nerve by the lesser saphenous vein and the fascia.
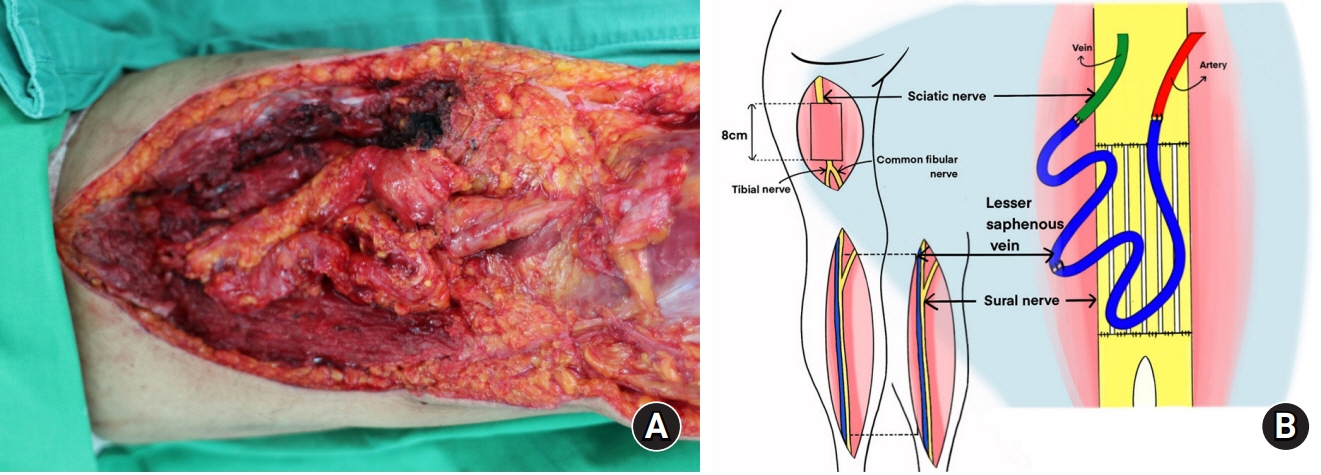
Fig. 5. Repair of the sciatic nerve with the harvested bilateral vascularized sural nerve and vascular anastomosis at three sites, between two lesser saphenous veins, between the lesser saphenous vein and alongside the artery, and between the lesser saphenous vein and alongside the vein. (A) Intraoperative image. (B) Schematic diagram.
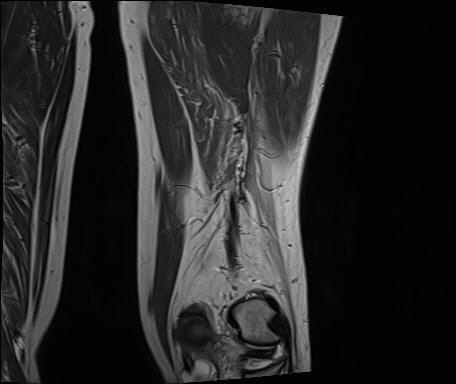
Fig. 6. Magnetic resonance image of the left posterior thigh at 20 months postsurgery shows no recurrence.
Reference
-
References
1. Grinsell D, Keating CP. Peripheral nerve reconstruction after injury: a review of clinical and experimental therapies. Biomed Res Int. 2014; 2014:698256.
Article2. Taylor GI, Ham FJ. The free vascularized nerve graft. A further experimental and clinical application of microvascular techniques. Plast Reconstr Surg. 1976; 57:413–26.3. Terzis JK, Kostopoulos VK. Vascularized nerve grafts and vascularized fascia for upper extremity nerve reconstruction. Hand (N Y). 2010; 5:19–30.
Article4. Burks SS, Levi DJ, Hayes S, Levi AD. Challenges in sciatic nerve repair: anatomical considerations. J Neurosurg. 2014; 121:210–8.
Article5. Doi K, Tamaru K, Sakai K, Kuwata N, Kurafuji Y, Kawai S. A comparison of vascularized and conventional sural nerve grafts. J Hand Surg Am. 1992; 17:670–6.
Article6. Mackinnon SE, Kelly L, Hunter DA. Comparison of regeneration across a vascularized versus conventional nerve graft: case report. Microsurgery. 1988; 9:226–34.
Article7. D’Arpa S, Claes KE, Stillaert F, Colebunders B, Monstrey S, Blondeel P. Vascularized nerve "grafts": just a graft or a worthwhile procedure? Plast Aesthet Res. 2015; 2:183–94.
Article8. Kline DG, Kim D, Midha R, Harsh C, Tiel R. Management and results of sciatic nerve injuries: a 24-year experience. J Neurosurg. 1998; 89:13–23.
Article9. Gaul JS Jr. Intrinsic motor recovery--a long-term study of ulnar nerve repair. J Hand Surg Am. 1982; 7:502–8.
Article10. Nicholson OR, Seddon HJ. Nerve repair in civil practice; results of treatment of median and ulnar nerve lesions. Br Med J. 1957; 2:1065–71.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sural Nerve Graftafter Resection of a Schwannoma in the Sciatic Nerve : A Case Report
- Combined Femoral and Sciatic Nerve Palsy Associated with Acetabular Fracture and Dislocation: A Case Report
- Effect of Partial Sciatic Nerve Injury on the Response to Formalin Test in Rats
- Sural nerve grafts in subacute facial nerve injuries: a report of two cases
- Experimental Study on Nerve Regeneration Using Reversed Vascularized Nerve Graft
