Surgical treatment of sagittal band injuries and classification according to operative findings
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Gwangmyeong Sungae General Hospital, Gwangmyeong, Korea
- KMID: 2526647
- DOI: http://doi.org/10.12790/ahm.21.0135
Abstract
- Purpose
The indications for surgery in patients with acute closed sagittal band injuries are still undetermined. The purpose of this study was to classify the types of injuries based on intraoperative findings of patients who underwent surgery for sagittal injuries, and to present the treatment plans and surgical methods.
Methods
Twenty-five patients who had undergone surgical exploration for closed sagittal band injuries between January 2011 and December 2020 were included in the study, comprising 17 patients with acute injuries (within 3 weeks), four patients with chronic injuries, and four patients who underwent surgery because symptoms did not improve in response to conservative treatment. Patients with laceration, fracture, and rheumatoid arthritis were excluded.
Results
Sagittal band injuries were classified into two groups: superficial sagittal band (SSB) and proper sagittal band (PSB) injuries. SSB injuries were observed in 75.0% of spontaneous rupture cases and PSB injuries were observed in 66.7% of traumatic rupture cases. SSB injuries were observed in 83.3% of Rayan and Murray classification type II cases and PSB injuries were observed in 61.5% of type III cases (p=0.041). PSB injuries were present in all four patients who underwent surgery because conservative treatment failed.
Conclusion
We successfully corrected sagittal band injuries with extensor digitorum communis tendon instability through surgical treatment. Sagittal band injuries can be classified into two types depending on the anatomical injury pattern; SSB and PSB injuries. The surgical method and treatment plan can be chosen based on this classification.
Figure
-

Fig. 1. Superficial sagittal band injury. (A) Tear of the superficial layer of the radial sagittal band is noted intraoperatively. With the metacarpophalangeal joint in an extended state, the extensor digitorum communis (EDC) tendon (asterisk) remains in place. (B) The forceps are holding the EDC tendon (asterisk). The EDC tendon is detached from the deep layer. The deep layers beneath the EDC tendon and the proper sagittal band (arrow) on the radial side are intact.

Fig. 2. Proper sagittal band (PSB) injury. (A) Complete rupture with gap formation on the ulnar side PSB (arrow) is noted intraoperatively. With the metacarpophalangeal joint flexed at approximately 15°, the gap widens and the extensor digitorum communis (EDC) tendon (asterisk) is displaced radially as a unit with the extensor hood. (B) The forceps are holding the thick PSB (arrow). The EDC tendon (asterisk) is completely covered by a superficial layer and a deep layer.
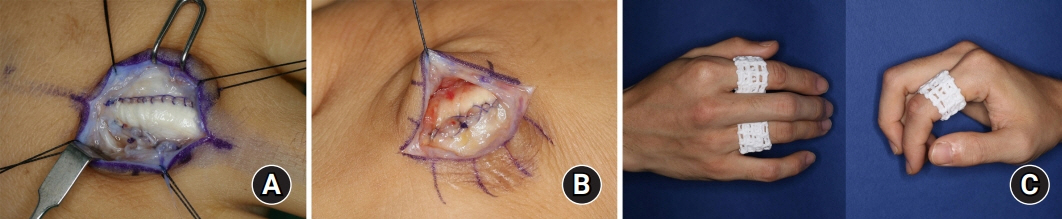
Fig. 3. (A) The superficial sagittal band injury is slightly and loosely repaired using a paratendon PDS 5-0 suture (Ethicon, Inc., Somerville, NJ, USA) at the border of the extensor digitorum communis tendon. (B) In a case of proper sagittal band (PSB) injury, the ruptured PSB is substantially repaired to prevent gap widening through the multiple figure-of-eight method and the consecutive method using PDS 4-0 and PDS 5-0 sutures.
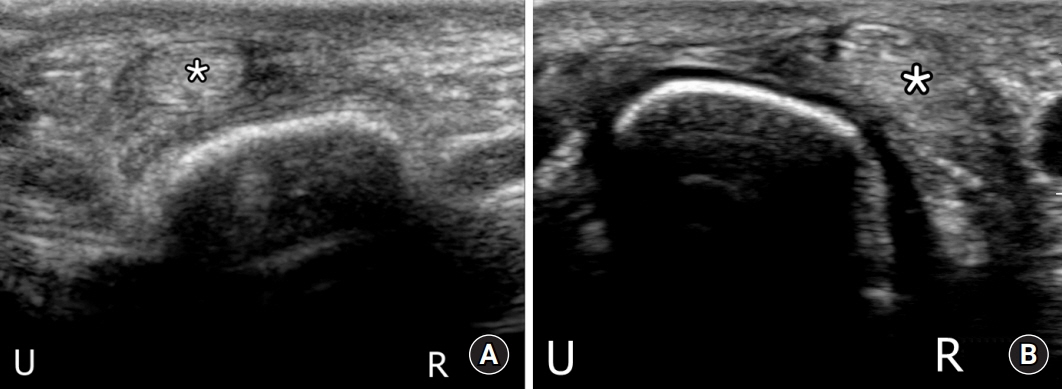
Fig. 4. (A) Preoperative ultrasonography (USG) of a superficial sagittal band injury. Axial dynamic view of the third metacarpophalangeal (MP) joint during flexion shows hypoechoic thickening on the radial side of the extensor digitorum communis (EDC) tendon (asterisk). The EDC tendon is subluxed to the ulnar side. (B) Preoperative USG of a proper sagittal band (PSB) injury. Axial dynamic view of the third MP joint during flexion shows radial dislocation of the EDC tendon (asterisk). R, radial; U, ulnar.

Fig. 5. Treatment algorithm for sagittal band injuries. SSB, superficial sagittal band; PSB, proper sagittal band.
Reference
-
References
1. Kichouh M, Vanhoenacker F, Jager T, et al. Functional anatomy of the dorsal hood or the hand: correlation of ultrasound and MR findings with cadaveric dissection. Eur Radiol. 2009; 19:1849–56.
Article2. Kleinhenz BP, Adams BD. Closed sagittal band injury of the metacarpophalangeal joint. J Am Acad Orthop Surg. 2015; 23:415–23.
Article3. Rayan GM, Murray D. Classification and treatment of closed sagittal band injuries. J Hand Surg Am. 1994; 19:590–4.
Article4. Ishizuki M. Traumatic and spontaneous dislocation of extensor tendon of the long finger. J Hand Surg Am. 1990; 15:967–72.
Article5. Kichouh M, De Maeseneer M, Jager T, Marcelis S, Van Hedent E, De Mey J. The thickness of the sagittal bands in volunteers: high resolution ultrasound of the fingers. Surg Radiol Anat. 2011; 33:65–70.
Article6. Willekens I, Kichouh M, Boulet C, De Maeseneer M, Clarys JP, de Mey J. Ultrasound follow-up of posttraumatic injuries of the sagittal band of the dorsal hood treated by a conservative approach. Eur J Radiol. 2015; 84:278–83.
Article7. Hong IT, Oh CH, Sim YS, Han SH. Direct repair of the sagittal band for extensor tendon subluxation caused by finger flicking. Orthopade. 2017; 46:755–60.
Article8. Kilgore ES, Graham WP, Newmeyer WL, Brown LG. Correction of ulnar subluxation of the extensor communis. Hand. 1975; 7:272–4.
Article9. Wheeldon FT. Recurrent dislocation of extensor tendons in the hand. J Bone Joint Surg Br. 1954; 36-B:612–7.
Article10. Koniuch MP, Peimer CA, VanGorder T, Moncada A. Closed crush injury of the metacarpophalangeal joint. J Hand Surg Am. 1987; 12(5 Pt 1):750–7.
Article11. Araki S, Ohtani T, Tanaka T. Acute dislocation of the extensor digitorum communis tendon at the metacarpophalangeal joint. A report of five cases. J Bone Joint Surg Am. 1987; 69:616–9.
Article12. Inoue G, Tamura Y. Dislocation of the extensor tendons over the metacarpophalangeal joints. J Hand Surg Am. 1996; 21:464–9.
Article13. Catalano LW 3rd, Gupta S, Ragland R 3rd, Glickel SZ, Johnson C, Barron OA. Closed treatment of nonrheumatoid extensor tendon dislocations at the metacarpophalangeal joint. J Hand Surg Am. 2006; 31:242–5.
Article14. Ritts GD, Wood MB, Engber WD. Nonoperative treatment of traumatic dislocations of the extensor digitorum tendons in patients without rheumatoid disorders. J Hand Surg Am. 1985; 10:714–6.
Article15. Carroll C 4th, Moore JR, Weiland AJ. Posttraumatic ulnar subluxation of the extensor tendons: a reconstructive technique. J Hand Surg Am. 1987; 12:227–31.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chronic Injury of Sagittal Band by Metacarpal Head Osteoma: A Case Report
- The Treatment of Acromioclavicular Seperation
- A Clinical Study of Fractures and Fracture - Dislocations of the Thoracolumbar Spine Injuries
- The Treatment of Acromioclavicular separation
- A Repair of Sagittal Band for Subluxation of the Extensor Tendons at the Metacarpophalangeal Joint
