Xanthomatous Hypophysitis Secondary to a Ruptured Rathke’s Cleft Cyst: A Case Report
- Affiliations
-
- 1Departments of Endocrinology and Metabolism, Faculty of Medicine, Kocaeli University, Kocaeli, Turkey
- 2Departments of Neurosurgery, Faculty of Medicine, Kocaeli University, Kocaeli, Turkey
- 3Departments of Pathology, Faculty of Medicine, Kocaeli University, Kocaeli, Turkey
- KMID: 2525303
- DOI: http://doi.org/10.14791/btrt.2022.10.e24
Abstract
- Hypophysitis (HP) is a rare disease which develops secondary to chronic or acute inflammation of the pituitary gland and may cause symptoms related to pituitary dysfunction and mass compression. Lymphocytic HP is the most common subtype of primary HP, while xanthomatous HP (XHP) is considered the rarest form, with 35 reported cases, to date. A 35-year-old woman was initially admitted to a Gynecology clinic with a 2-year history of amenorrhea and headache. She was started on cabergoline 0.5 mg twice a week for macroprolactinoma. Due to persistent amenorrhea with low gonadotropins, she was referred to our Endocrinology clinic. Her pituitary function profile revealed panhypopituitarism and a 13×11×12 mm sized sellar mass with diffuse enhancement which sustained toward the infundibulum and dura was observed on the gadolinium-enhanced pituitary MRI. The patient underwent an endoscopic endonasal transsphenoidal approach for tumor resection and thick yellowish fluid draining from the lesion was observed. The histopathological diagnosis was reported as a rupture of an Rathke’s cleft cyst and an XHP. The surgery did not improve the symptoms/pituitary functions, however, headache recovered immediately after the first dose of high dose methylprednisolone treatment. The inflammatory process in a xanthomatous lesion may actually be a secondary response to mucous fluid content release from a ruptured cyst, thus recommended to classify XHP as secondary hypophysitis. Since the differentiation of XHP from other pituitary tumors may be challenging preoperatively, surgery is the major diagnostic tool and also, the most recommended therapeutic option.
Figure
-
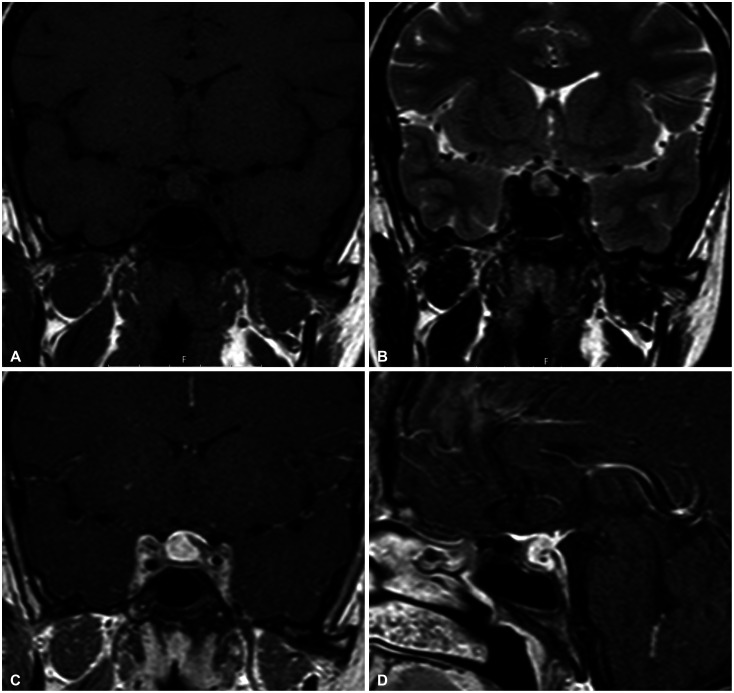
Fig. 1 Preoperative gadolinium-enhanced MRI scan of xanthomatous hypophysitis secondary to Rathke’s cleft cyst. A: Pre-contrast coronal T1-weighted MR image. B: Coronal T2-weighted MR image. C: Post-contrast coronal. D: Sagittal T1-weighted MR images of the pituitary lesion.
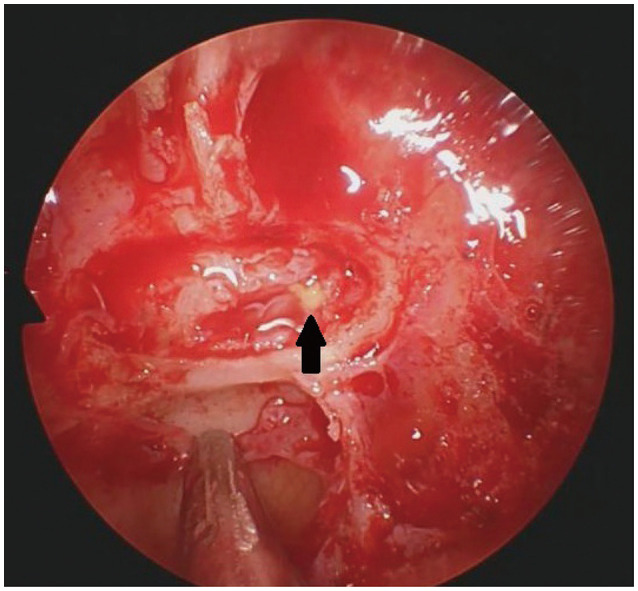
Fig. 2 Intraoperative image demonstrating thick yellowish fluid draining (arrow) from the pituitary lesion.
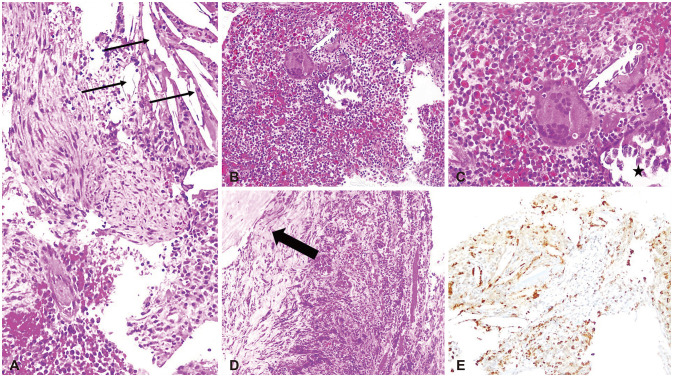
Fig. 3 Histological images of the resected pituitary lesion. A: Numerous cholesterol clefts (arrows) in sections obtained from the pituitary mass (H&E, ×200). B: An area of lymphoplasmacytic cells with multinucleate giant cells and microcalcification (H&E, ×100). C: Numerous foamy and hemosiderin-containing macrophages with admixed lymphocytes and histiocytes (asterisk) and higher magnification of the B (H&E, ×200). D: Dense fibrous tissues containing chronic inflammatory cells (arrow) (H&E, ×100). E: Histiocytes stained positively with CD68 (CD68, ×100).
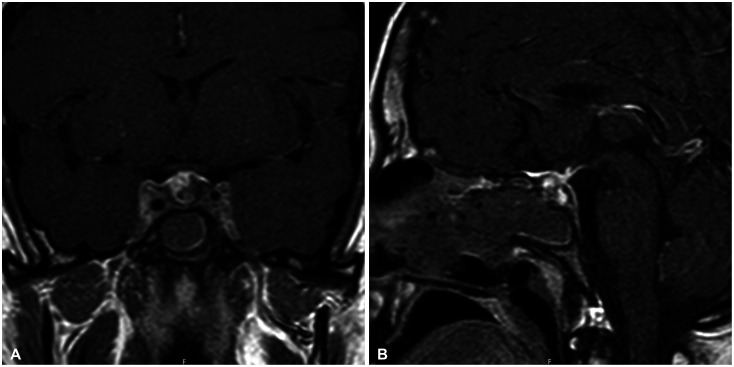
Fig. 4 Postoperative gadolinium-enhanced MRI scan of the sellar area. Post-contrast coronal (A) and sagittal (B) T1-weighted MR images of the pituitary region.
Reference
-
1. Angelousi A, Alexandraki K, Tsoli M, Kaltsas G, Kassi E. Hypophysitis (including IgG4 and immunotherapy). Neuroendocrinology. 2020; 110:822–835. PMID: 32126548.
Article2. Caranci F, Leone G, Ponsiglione A, Muto M, Tortora F, Muto M, et al. Imaging findings in hypophysitis: a review. Radiol Med. 2020; 125:319–328. PMID: 31863360.
Article3. Faje A. Hypophysitis: evaluation and management. Clin Diabetes Endocrinol. 2016; 2:15. PMID: 28702249.
Article4. Gubbi S, Hannah-Shmouni F, Verbalis JG, Koch CA. Hypophysitis: an update on the novel forms, diagnosis and management of disorders of pituitary inflammation. Best Pract Res Clin Endocrinol Metab. 2019; 33:101371. PMID: 31866206.5. Mathkour M, Zeoli T, Werner C, Scullen T, Garces J, Keen J, et al. Recurring primary xanthomatous hypophysitis behaving like pituitary adenoma: additional case and literature review. World Neurosurg. 2020; 138:27–34. PMID: 32081821.6. Hanna B, Li YM, Beutler T, Goyal P, Hall WA. Xanthomatous hypophysitis. J Clin Neurosci. 2015; 22:1091–1097. PMID: 25957783.
Article7. Oishi M, Hayashi Y, Fukui I, Kita D, Miyamori T, Nakada M. Xanthomatous hypophysitis associated with autoimmune disease in an elderly patient: a rare case report. Surg Neurol Int. 2016; 7:S449–S453. PMID: 27500004.
Article8. Aste L, Bellinzona M, Meleddu V, Farci G, Manieli C, Godano U. Xanthomatous hypophysitis mimicking a pituitary adenoma: case report and review of the literature. J Oncol. 2010; 2010:195323. PMID: 20671950.
Article9. Joung JY, Jeong H, Cho YY, Huh K, Suh YL, Kim KW, et al. Steroid responsive xanthomatous hypophysitis associated with autoimmune thyroiditis: a case report. Endocrinol Metab (Seoul). 2013; 28:65–69. PMID: 24396654.
Article10. Singh K, Kanodia AK, Ross P, Torgersen A, Maclean J, Leese G, et al. Xanthomatous hypophysitis causing hypogonadotropic hypogonadism resulting in delayed presentation of slipped capital femoral epiphysis. Br J Neurosurg. 2018; 11. 19. [Epub]. Available at: . DOI: 10.1080/02688697.2018.1525482.
Article11. Duan K, Asa SL, Winer D, Gelareh Z, Gentili F, Mete O. Xanthomatous hypophysitis is associated with ruptured Rathke’s cleft cyst. Endocr Pathol. 2017; 28:83–90. PMID: 28120170.12. Kleinschmidt-DeMasters BK, Lillehei KO, Hankinson TC. Review of xanthomatous lesions of the sella. Brain Pathol. 2017; 27:377–395. PMID: 28236350.13. Folkerth RD, Price DL Jr, Schwartz M, Black PM, De Girolami U. Xanthomatous hypophysitis. Am J Surg Pathol. 1998; 22:736–741. PMID: 9630181.
Article14. Niyazoglu M, Celik O, Bakkaloglu DV, Oz B, Tanriöver N, Gazioglu N, et al. Xanthomatous hypophysitis. J Clin Neurosci. 2012; 19:1742–1744. PMID: 22682648.15. Gutenberg A, Hans V, Puchner MJ, Kreutzer J, Brück W, Caturegli P, et al. Primary hypophysitis: clinical-pathological correlations. Eur J Endocrinol. 2006; 155:101–107. PMID: 16793955.16. Burt MG, Morey AL, Turner JJ, Pell M, Sheehy JP, Ho KK. Xanthomatous pituitary lesions: a report of two cases and review of the literature. Pituitary. 2003; 6:161–168. PMID: 14971740.17. Komatsu F, Tsugu H, Komatsu M, Sakamoto S, Oshiro S, Fukushima T, et al. Clinicopathological characteristics in patients presenting with acute onset of symptoms caused by Rathke’s cleft cysts. Acta Neurochir (Wien). 2010; 152:1673–1678. PMID: 20495985.18. Sonnet E, Roudaut N, Mériot P, Besson G, Kerlan V. Hypophysitis associated with a ruptured Rathke’s cleft cyst in a woman, during pregnancy. J Endocrinol Invest. 2006; 29:353–357. PMID: 16699303.19. Miyajima Y, Oka H, Utsuki S, Fujii K. Rathke’s cleft cyst with xanthogranulomatous change--case report. Neurol Med Chir (Tokyo). 2011; 51:740–742. PMID: 22027255.20. Amano K, Kubo O, Komori T, Tanaka M, Kawamata T, Hori T, et al. Clinicopathological features of sellar region xanthogranuloma: correlation with Rathke’s cleft cyst. Brain Tumor Pathol. 2013; 30:233–241. PMID: 23322180.21. Schittenhelm J, Beschorner R, Psaras T, Capper D, Nägele T, Meyermann R, et al. Rathke’s cleft cyst rupture as potential initial event of a secondary perifocal lymphocytic hypophysitis: proposal of an unusual pathogenetic event and review of the literature. Neurosurg Rev. 2008; 31:157–163. PMID: 18253771.22. Cheung CC, Ezzat S, Smyth HS, Asa SL. The spectrum and significance of primary hypophysitis. J Clin Endocrinol Metab. 2001; 86:1048–1053. PMID: 11238484.23. Hama S, Arita K, Nishisaka T, Fukuhara T, Tominaga A, Sugiyama K, et al. Changes in the epithelium of Rathke cleft cyst associated with inflammation. J Neurosurg. 2002; 96:209–216. PMID: 11838792.24. Nishikawa T, Takahashi JA, Shimatsu A, Hashimoto N. Hypophysitis caused by Rathke’s cleft cyst. Case report. Neurol Med Chir (Tokyo). 2007; 47:136–139. PMID: 17384498.25. Wong JSL, Nasruddin AB, Selveindran NM, Latif KA, Kassim F, Nair SB, et al. Xanthomatous hypophysitis presenting in an adolescent girl: a long-term follow-up of a rare case and review of the literature. AACE Clin Case Rep. 2021; 7:220–225. PMID: 34095493.26. Lin W, Gao L, Guo X, Wang W, Xing B. Xanthomatous hypophysitis presenting with diabetes insipidus completely cured through transsphenoidal surgery: case report and literature review. World Neurosurg. 2017; 104:1051.e7–1051.e13.
