Curious Case of Acoustic Schwannoma of Middle Cranial Fossa: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, Max Super Speciality Hospital, Patparganj, New Delhi, India
- KMID: 2525302
- DOI: http://doi.org/10.14791/btrt.2022.10.e21
Abstract
- Acoustic neuromas are the most common lesion in the cerebellopontine angle. The authors report a unique case of acoustic schwannoma, presenting in middle cranial fossa masquerading as meningioma in a 24-year-old man, presenting with headache and focal seizures. Contrast-enhanced MRI of the brain revealed a mass lesion of the right middle cranial fossa consistent with features of meningioma.Intraoperatively a well-defined tumor with attachment to anterior petrous bone was excised. In the immediate postoperative period, the patient developed right-sided hearing loss, which was proven to be retrochoclear hearing loss on brainstem evoked response audiometry. Histopathology findings were consistent with benign schwannoma. Acoustic schwannoma originating in an unusual location middle cranial fossa is a plausible explanation of such unusual occurrence. Such a case has never been reported in the literature.
Figure
-
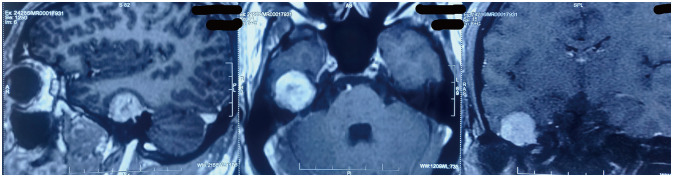
Fig. 1 Contrast-enhanced MRI sagittal, axial, and coronal sections showing tumor arising from right middle cranial fossa.

Fig. 2 Histopathological finding. A: H&E section (×10) shows a biphasic tumor comprised of oval to spindle shaped cells with cellular component (Antoni A area) and myxoid hypocellular component (Antoni B area). B: H&E section (×40) shows tumor comprised of cells are narrow, elongated and wavy with tapered ends interspersed with collagen fibers with an occasional mitotic figure. C: Section examined shows diffuse strong (4+) cytoplasmic positivity of tumor cells for vimentin on immunohistochemistry (×40). D: Section examined shows diffuse cytoplasmic and focal nuclear positivity of tumor cells for S-100 on immunohistochemistry (×10).

Fig. 3 Postoperative noncontrast CT showing erosion of right petrous bone at the site of attachment of tumor.
Reference
-
1. Sanna M, Mancini F, Russo A, Taibah A, Falcioni M, Di Trapani G. Atlas of acoustic neurinoma microsurgery. 2nd ed. Stuttgart: Thieme;2011.2. Silk PS, Lane JI, Driscoll CL. Surgical approaches to vestibular schwannomas: what the radiologist needs to know. Radiographics. 2009; 29:1955–1970. PMID: 19926756.
Article3. Kumar V, Abbas AK, Aster JC. Robbins and Cotran pathologic basis of disease. 9th ed. Philadelphia: Elsevier Saunders;2015.4. Lanser MJ, Sussman SA, Frazer K. Epidemiology, pathogenesis, and genetics of acoustic tumors. Otolaryngol Clin North Am. 1992; 25:499–520. PMID: 1625863.
Article5. Russels DS, Rubinstein LJ. Pathology of tumors of the nervous system. 5th ed. London: Edward Arnold;1989.6. Gao Y, Qin Z, Li D, Yu W, Sun L, Liu N, et al. Intracerebral schwannoma: a case report and literature review. Oncol Lett. 2018; 16:2501–2510. PMID: 30013644.
Article7. Rotondo M, Pascale M, Scuotto A. Giant frontal intraparenchymal schwannoma: unexpected diagnosis. BMJ Case Rep. 2013; 2013:bcr2013010350.8. Bansal AK, Bindal R, Shetty DC, Dua M. Rare occurrence of intraosseous schwannoma in a young child, its review and its pathogenesis. J Oral Maxillofac Pathol. 2012; 16:91–96. PMID: 22438647.
Article9. Rais F, Benhmidou N, Rais G, Kouhen F, Bellahamou K, Loughlimi H, et al. Solitary intraosseous schwannoma of the base and vault of the skull: a summary review of such unusual location. Clin Sarcoma Res. 2015; 5:6. PMID: 25667745.10. Jackler RK, Parker DA. Radiographic differential diagnosis of petrous apex lesions. Am J Otol. 1992; 13:561–574. PMID: 1449185.11. Feghali JG, Kantrowitz AB. Atypical invasion of the temporal bone in vestibular schwannoma. Skull Base Surg. 1995; 5:33–36. PMID: 17171155.
Article12. Park SJ, Yang NR, Seo EK. Vestibular schwannoma atypically invading temporal bone. J Korean Neurosurg Soc. 2015; 57:292–294. PMID: 25932298.13. Patankar AP, Sheth JH. Intracranial malignant nerve sheath tumor in the middle cranial fossa: a rare case report with review of literature. Asian J Neurosurg. 2019; 14:922–926. PMID: 31497130.14. Ziadi A, Saliba I. Malignant peripheral nerve sheath tumor of intracranial nerve: a case series review. Auris Nasus Larynx. 2010; 37:539–545. PMID: 20399579.15. L’heureux-Lebeau B, Saliba I. Updates on the diagnosis and treatment of intracranial nerve malignant peripheral nerve sheath tumors. Onco Targets Ther. 2013; 6:459–470. PMID: 23667313.16. Watanabe T, Saito N, Sato N, Takahashi A, Fujimaki H, Tosaka M, et al. High incidence and spontaneous resolution of mastoid effusion after craniotomy on early postoperative magnetic resonance images. Neuroradiology. 2003; 45:482–488. PMID: 12811440.17. Ying T, Thirumala P, Gardner P, Habeych M, Crammond D, Balzer J. The incidence of early postoperative conductive hearing loss after microvascular decompression of hemifacial spasm. J Neurol Surg B Skull Base. 2015; 76:411–415. PMID: 26682118.18. Uppar AM, Rao S, Prasad C, Arimappamagan A, Santosh V. Schwannoma of the greater superficial petrosal nerve: an unusual site for a common tumor. J Neurol Surg A Cent Eur Neurosurg. 2020; 81:565–570. PMID: 32361981.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Vestibular Schwannoma Treated with Revision Middle Cranial Fossa Approach to Preserve Facial Nerve Function and Hearing Ability
- A Case of Facial Nerve Schwannoma Extending into the Middle Cranial Fossa
- A Case of Image-Guided Acoustic Neuroma Surgery via Middle Cranial Fossa Approach
- Middle cranial fossa tumors of rare and atypical CT features
- A Case of Vestibular Schwannoma with Acute Spontaneous Vertigo
