Endoscopic Management of Anastomotic Leakage after Esophageal Surgery: Ten Year Analysis in a Tertiary University Center
- Affiliations
-
- 1Department for General - and Visceral Surgery, University Hospital, Klinikum Oldenburg AöR, Germany
- 2Department for Internal Medicine and Gastroenterology, University Hospital, Klinikum Oldenburg AöR, Germany
- KMID: 2525051
- DOI: http://doi.org/10.5946/ce.2021.099
Abstract
- Background/Aims
Anastomotic leakage after esophageal surgery remains a feared complication. During the last decade, management of this complication changed from surgical revision to a more conservative and endoscopic approach. However, the treatment remains controversial as the indications for conservative, endoscopic, and surgical approaches remain non-standardized.
Methods
Between 2010 and 2020, all patients who underwent Ivor Lewis esophagectomy for underlying malignancy were included in this study. The data of 28 patients diagnosed with anastomotic leak were further analyzed.
Results
Among 141 patients who underwent resection, 28 (19.9%) developed an anastomotic leak, eight (28.6%) of whom died. Thirteen patients were treated with endoluminal vacuum therapy (EVT), seven patients with self-expanding metal stents (SEMS) four patients with primary surgery, one patient with a hemoclip, and three patients were treated conservatively. EVT achieved closure in 92.3% of the patients with a large defect and no EVT-related complications. SEMS therapy was successful in clinically stable patients with small defect sizes.
Conclusions
EVT can be successfully applied in the treatment of anastomotic leakage in critically ill patients, while SEMS should be limited to clinically stable patients with a small defect size. Surgery is only warranted in patients with sepsis with graft necrosis.
Keyword
Figure
-

Fig. 1. Management of anastomotic leakage by endoluminal vacuum therapy (EVT). A 75-year-old patient with ypT3 pN1 M0 R0 Barrett’s carcinoma treated with thoracoabdominal esophagectomy after neoadjuvant chemotherapy. (A, B) An approximately 3-cm large anastomotic leakage cavity on the 10th postoperative day in which deeper fistulas could be excluded. (C, D) After EVT for 10 days, there was a clear tendency towards granulation. (E) The insufficiency cavity was significantly smaller and the EVT was completed after 14 days. (F) Endoscopic control after a total of 24 days showed an almost closed insufficiency.
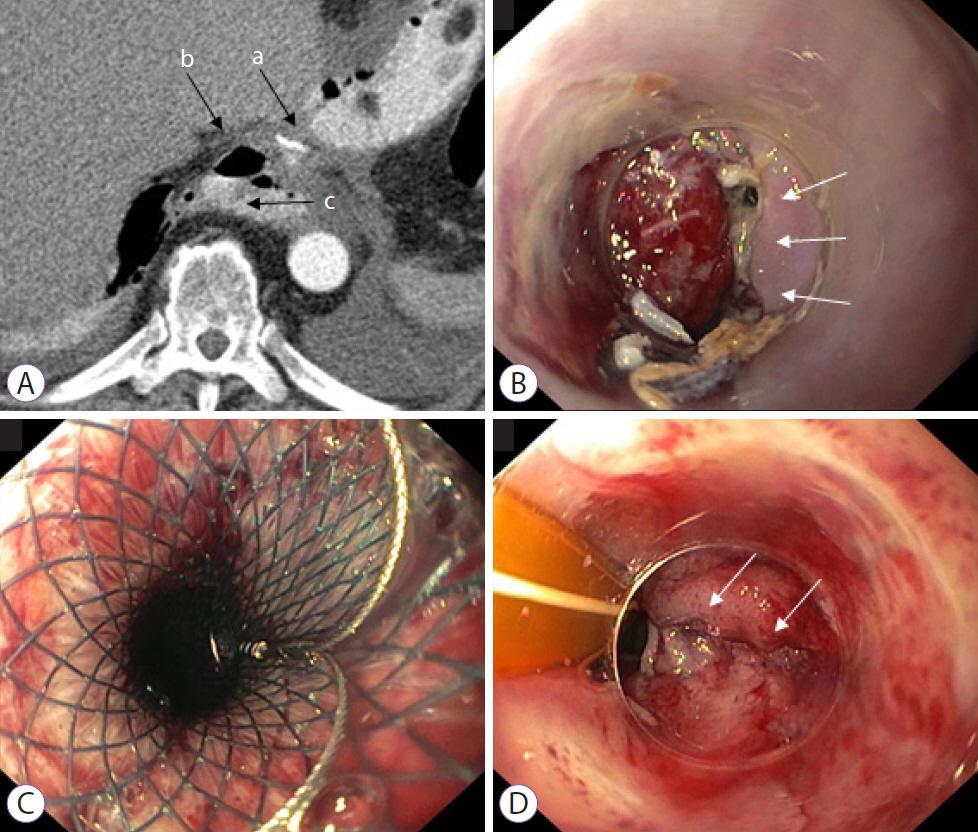
Fig. 2. Management of anastomotic leakage using a self-expanding metal stent (SEMS). A 67-year-old patient with pT1b (sm1) pN0 M0 R0 adenocarcinoma was treated with transhiatal distal esophagectomy. (A) CT scan in the region of the anastomosis (a) with detection of extraluminal free air (b) and contrast medium (c) on the 7th postoperative day. (B) Endoscopy with detection of an approximately 6-mm small anastomotic leakage with an otherwise vital anastomosis. (C) In the absence of evidence for an abscess, a fully covered self-expanding metal stent with a diameter of 28 mm was implanted. (D) The stent was removed after three weeks. The small anastomotic leakage was almost completely closed.

Fig. 3. Treatment algorithm for patients treated for anastomotic leak after esophagectomy. Of the 28 patients, 13 were treated with endoluminal vacuum therapy (EVT), seven with self-expanding metal stents (SEMS), one with a clip, three were treated conservatively, and four patients required surgery to treat the defect.
Reference
-
1. Ryan CE, Paniccia A, Meguid RA, McCarter MD. Transthoracic anastomotic leak after esophagectomy: current trends. Ann Surg Oncol. 2017; 24:281–290.2. El-Sourani N, Bruns H, Troja A, Raab H-R, Antolovic D. Routine use of contrast swallow after total gastrectomy and esophagectomy: is it justified? Pol J Radiol. 2017; 82:170–173.3. Hölscher AH, Vallböhmer D, Brabender J. The prevention and management of perioperative complications. Best Pract Res Clin Gastroenterol. 2006; 20:907–923.4. Karl RC, Schreiber R, Boulware D, Baker S, Coppola D. Factors affecting morbidity, mortality, and survival in patients undergoing Ivor Lewis esophagogastrectomy. Ann Surg. 2000; 231:635–643.5. Singh D, Maley RH, Santucci T, et al. Experience and technique of stapled mechanical cervical esophagogastric anastomosis. Ann Thorac Surg. 2001; 71:419–424.6. Michel L, Grillo HC, Malt RA. Operative and nonoperative management of esophageal perforations. Ann Surg. 1981; 194:57–63.7. Kuehn F, Loske G, Schiffmann L, Gock M, Klar E. Endoscopic vacuum therapy for various defects of the upper gastrointestinal tract. Surg Endosc. 2017; 31:3449–3458.8. Hünerbein M, Stroszczynski C, Moesta KT, Schlag PM. Treatment of thoracic anastomotic leaks after esophagectomy with self-expanding plastic stents. Ann Surg. 2004; 240:801–807.9. Truong S, Böhm G, Klinge U, Stumpf M, Schumpelick V. Results after endoscopic treatment of postoperative upper gastrointestinal fistulas and leaks using combined Vicryl plug and fibrin glue. Surg Endosc. 2004; 18:1105–1108.10. Doniec JM, Schniewind B, Kahlke V, Kremer B, Grimm H. Therapy of anastomotic leaks by means of covered self-expanding metallic stents after esophagogastrectomy. Endoscopy. 2003; 35:652–658.11. Wiedenhagen R, Spelsberg F, Lang RA, et al. New method for sepsis control caused by anastomotic leakage in rectal surgery: the Endo-VAC. Colorectal Dis. 2003; 5:1–4.12. Loske G, Schorsch T, Müller CT. Endoskopische Vakuumtherapie der akuten Mediastinitis: Ein modernes minimal-invasives Therapieverfahren. Chirurg. 2016; 87:790–792.13. Raju GS, Tarcin O. Endoscopic management of anastomotic esophageal leaks. Techniques in Gastrointestinal Endoscopy. 2006; 8:66–71.14. Pross M, Manger T, Reinheckel T, Mirow L, Kunz D, Lippert H. Endoscopic treatment of clinically symptomatic leaks of thoracic esophageal anastomoses. Gastrointest Endosc. 2000; 51:73–76.15. Schaible A, Schmidt T, Diener M, et al. Intrathoracic anastomotic leakage following esophageal and cardial resection: definition and validation of a new severity grading classification. Chirurg. 2018; 89:945–951.16. Schaheen L, Blackmon SH, Nason KS. Optimal approach to the management of intrathoracic esophageal leak following esophagectomy: a systematic review. Am J Surg. 2014; 208:536–543.17. Schniewind B, Schafmayer C, Voehrs G, et al. Endoscopic endoluminal vacuum therapy is superior to other regimens in managing anastomotic leakage after esophagectomy: a comparative retrospective study. Surg Endosc. 2013; 27:3883–3890.18. Schorsch T, Müller C, Loske G. Endoscopic vacuum therapy of anastomotic leakage and iatrogenic perforation in the esophagus. Surg Endosc. 2013; 27:2040–2045.19. Weidenhagen R, Hartl WH, Gruetzner KU, Eichhorn ME, Spelsberg F, Jauch KW. Anastomotic leakage after esophageal resection: new treatment options by endoluminal vacuum therapy. Ann Thorac Surg. 2010; 90:1674–1681.20. Jeon JH, Jang HJ, Han JE, et al. Endoscopic vacuum therapy in the management of postoperative leakage after esophagectomy. World J Surg. 2020; 44:179–185.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic management of postoperative upper gastrointestinal leakage
- Anastomotic Leakage and Stricture Relating to Anastomotic Level and Methods in Esophageal Resection and Reconstruction for Esophageal Cancer
- A Case of Endoscopic Stenting for Anastomotic Leakage after Total Gastrectomy
- Interrupted Single-layer Suture Technique in Esophageal Anastomosis Using Monofilament Polypropylene Suture
- Role of Endoscopic Vacuum Therapy as a Treatment for Anastomosis Leak after Esophageal Cancer Surgery
