A Ruptured Blood Blister-Like Aneurysm that Experienced Regrowth with Coil Compaction Twice in a Month : Case Report
- Affiliations
-
- 1Department of Neurosurgery, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan, Republic of Korea
- KMID: 2524666
- DOI: http://doi.org/10.7180/kmj.2021.36.2.200
Abstract
- Unlike other aneurysms, blood blister-like aneurysms(BBA) occur at non-branching sites, are commonly located at the dorsal wall of the supraclinoid internal carotid artery (ICA), and are suspected to arise from dissecting aneurysms. They are typically diagnosed after a bleed because of their small size and unusual site. Therefore, lesions exist after brain computed tomography or magnetic resonance imaging, but they are often not found. In the case of BBA, which have a high risk of recurrence, the treatment is difficult, and selecting the treatment method is also challenging. This paper describes the treatment of a BBA with internal trapping of the ICA that eventually recurred despite performing coil embolization twice.
Keyword
Figure
-
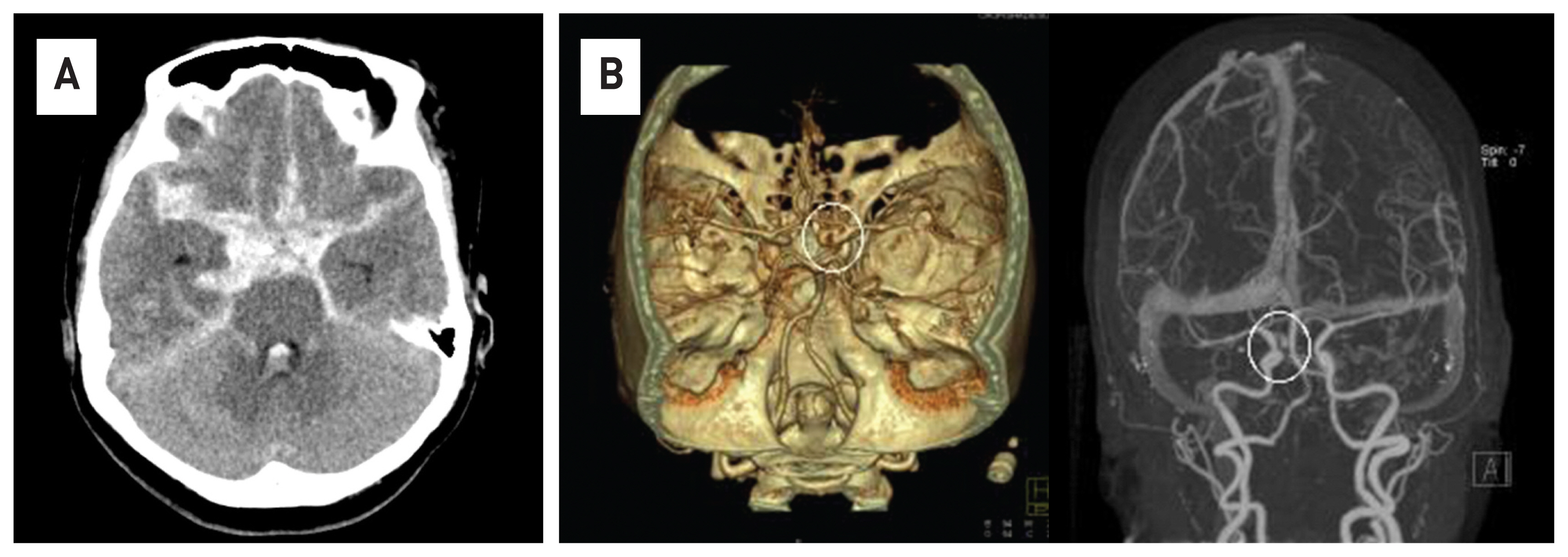
Fig. 1 Brain computed tomography(CT) scans show diffuse and thick subarachnoid hemorrhage in the basal cistern and both sylvian fissure (A). Contrast-enhanced CT angiography shows a cerebral aneurysm in the right distal ICA(white circle) (B).

Fig. 2 In the 4-vesselangiography, a ruptured cerebral aneurysm of a saccular type is observed on the dorsal wall of distal Internal cerebral artery(ICA)(white arrow)(A). The stent was deployed from the proximal ICA to the proximal middle cerebral artery, and the microcatheter was placed in the sac of aneurysm, and then coiling was performed (B). Endovascular coiling was densely packed into the aneurysm sac, and the procedure was terminated after confirming that there was no contrast filling with an aneurysm sac anymore
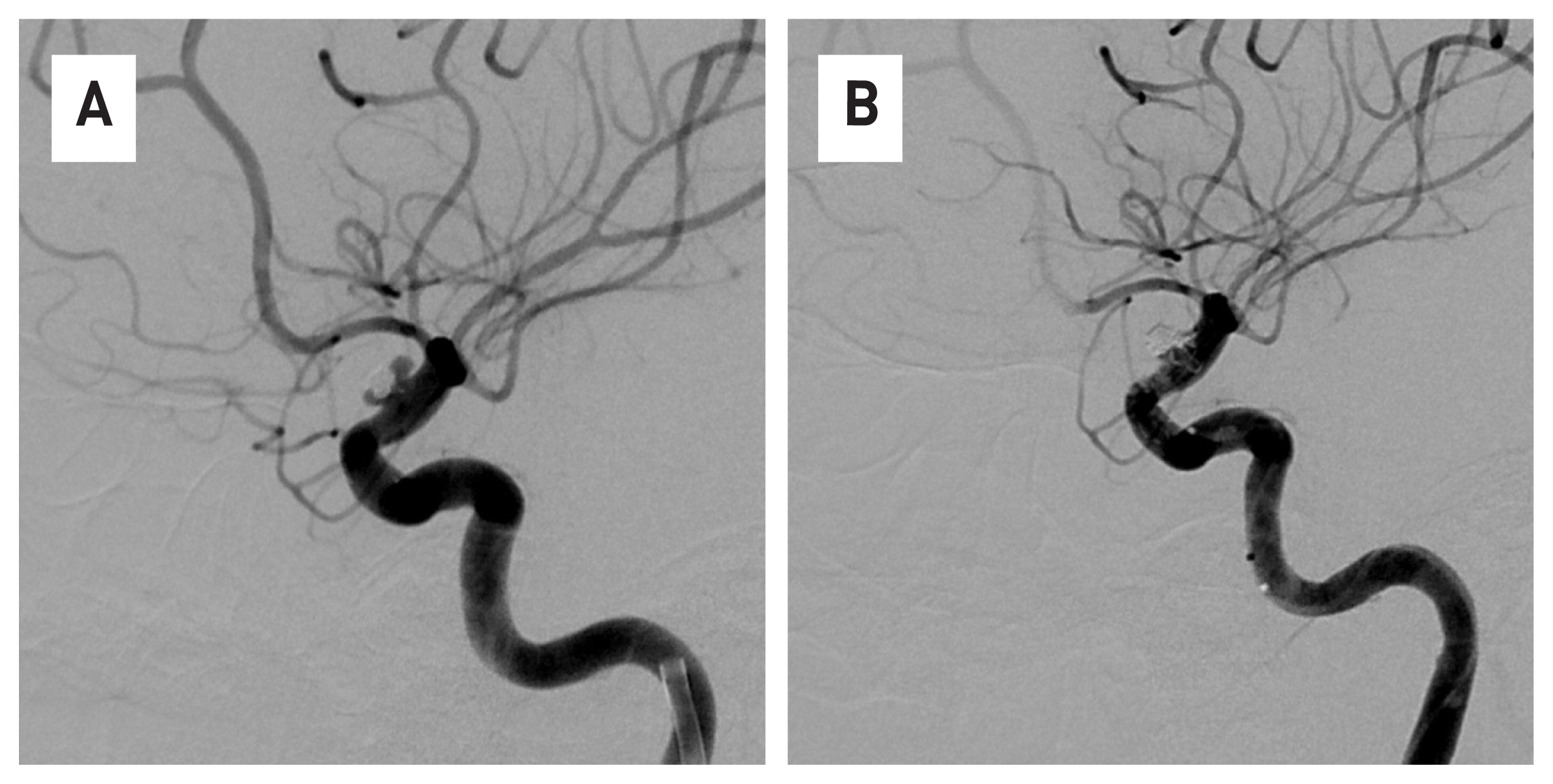
Fig. 3 The regrowth and coil compaction of aneurysm were observed in 4-vesselangiography two weeks after the first coil embolization (A). It was determined that additional treatment was necessary, endovascular coiling was performed on the recurrent aneurysm sac, and the procedure was terminated after checking the complete occlusion of the sac (B).

Fig. 4 The regrowth of cerebral aneurysm is observed again in 4-vesselangiography, which was performed two weeks after the additional procedure (A). Internal trapping treatment of distal internal cerebral artery was performed using coils (B). In the 4-vessel angiography conducted by the opposite internal cerebral artery, the flow of blood toward the lesion could be confirmed through anterior communicating artery (C).
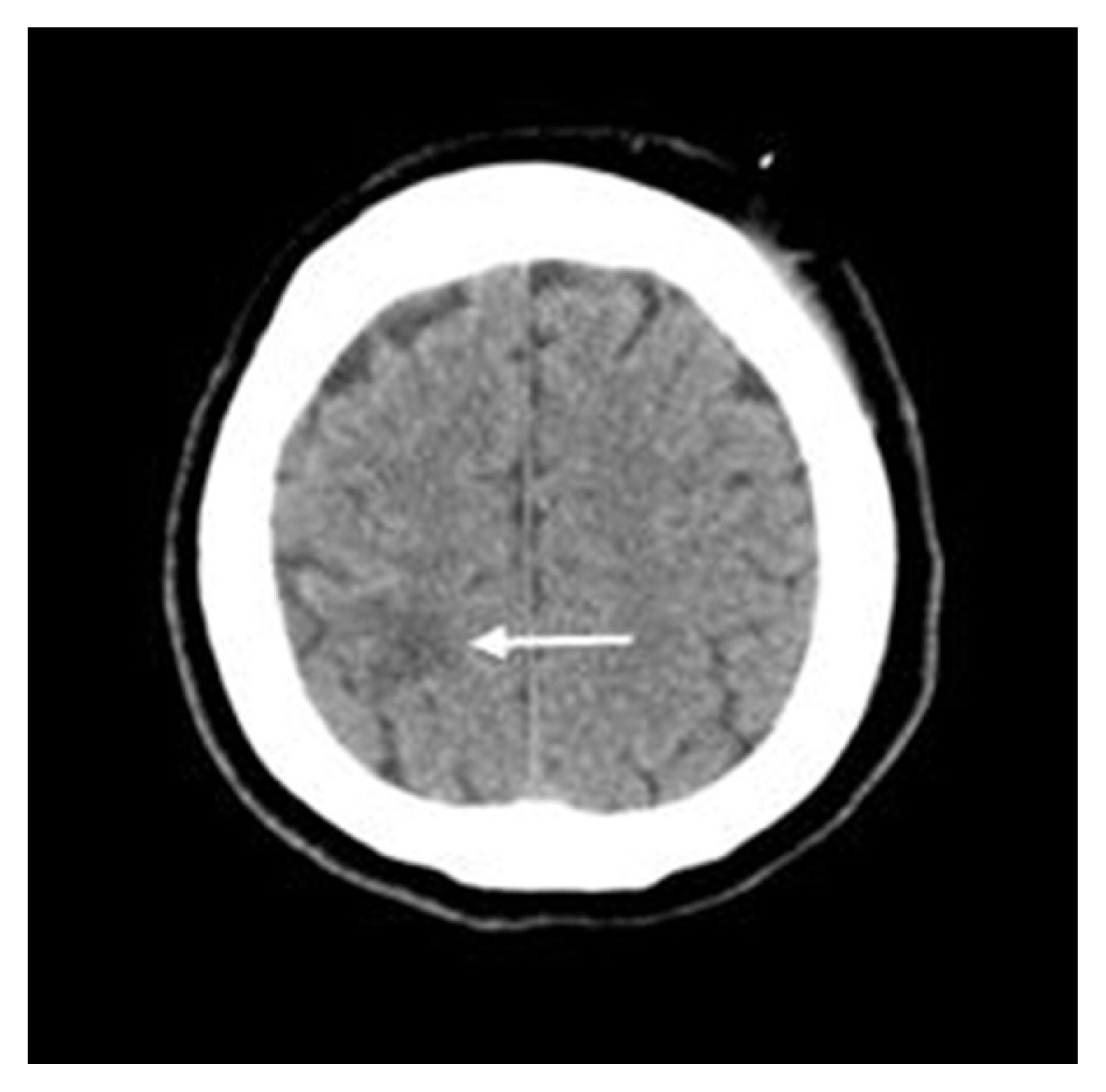
Fig. 5 After the second procedure, low density near the right motor cortex is observed and is thought to be a suspected cerebral infarction (white arrow).
Reference
-
1. Ahn JY, Cho JH, Jung JY, Lee BH, Yoon PH. Blister-like aneurysms of the supraclinoid internal carotid artery: challenging endovascular treatment with stent-assisted coiling. J ClinNeurosci. 2008; 15:1058–61.
Article2. Ahn JY, Kwon SO, Joo JY. Dorsal internal carotid artery aneurysm treated by coil embolization--case report. Neurol Med Chir (Tokyo). 2001; 41:603–5. discussion 606.3. Morris TC, Brophy BP. Blister-like aneurysm of the anterior communicating artery. J Clin-Neurosci. 2009; 16:1098–100.
Article4. Piotin M, Pistocchi S, Bartolini B, Blanc R. Intracranial aneurysm coiling with PGLA-coated coils versus bare platinum coils: long-term anatomic follow-up. Neuroradiology. 2012; 54:345–8.
Article5. Satoh A, Nakamura H, Odaki M, Kobayashi S, Kageyama Y, Fukuda K, et al. High risk aneurysms of the internal carotid artery: dorsal IC aneurysms. SurgCereb Stroke. 1993; 121:467–72.6. Kim BM, Kim DI, Chung EC, Kim SY, Shin YS, Park SI, et al. Endovascular coil embolization for anterior choroidal artery aneurysms. Neuroradiology. 2008; 50:251–7.
Article7. Lee BH, Kim BM, Park MS, Park SI, Chung EC, Suh SH, et al. Reconstructive endovascular treatment of ruptured blood blister-like aneurysms of the internal carotid artery. J Neurosurgery. 2009; 110:431–6.
Article8. Abe M, Tabuchi K, Yokoyama H, Uchino A. Blood blister like aneurysms of the internal carotid artery. J Neurosurgery. 1998; 89:419–24.9. Korja M, Rautio R, Valtonen S, Haapanen A. Primary treatment of ruptured blood blister-like aneurysms with stent-as sisted coil embolization: report of two cases. ActaRadiol. 2008; 49:180–3.10. Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet. 2002; 360:1267–74.
Article11. Andaluz N, Zuccarello M. Blister-like aneurysms of the anterior communicating artery. a retrospective review of diagnosis and treatment in five patients. Neurosurgery. 2008; 62:807–1. discussion 811.12. Meckel S, Singh TP, Undré P, Ramgren B, Nilsson OG, Phatouros C, et al. Endovascular treatment using predominantly stent-assisted coil embolization and antiplatelet and anticoagulation management of ruptured blood blister-like aneurysms. Am J Neuroradiol. 2011; 32:764–71.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Blood Blister-like Aneurysm Treated with Coil Embolization without Stent Assistance
- A Case of Ruptured Blood Blister-like Aneurysm Treated with Pipeline Embolization Device: Clinical Significance of Fetal-type Posterior Communicating Artery
- Coiling as Retreatment in Intracranial Aneurysm of de novo Formation or Regrowth: Case Report
- Electrothermal Coil Detachment Failure in Flow Diverter-Assisted Coiling of a Small Blister Aneurysm: Technical Considerations and Possible Solutions
- Microsurgical treatment for the recurrent cerebral aneurysm initially treated using coil embolization
