Kosin Med J.
2021 Dec;36(2):180-186. 10.7180/kmj.2021.36.2.180.
Removal of Large Urinary Stone Using Percutaneous Nephrolithotomy in a Patient with Crohn's Disease
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Republic of Korea
- KMID: 2524663
- DOI: http://doi.org/10.7180/kmj.2021.36.2.180
Abstract
- Extraintestinal manifestation (EIM) of inflammatory bowel disease (IBD) is approximately 36%. Of genitourinary complications as an EIM of Crohn’s disease (CD), nephrolithiasis is the most common urinary complication in patients with CD. CD patients have been shown to have decreased urinary volume, pH, magnesium, and excretion of citrate, all of which are significant risk factors for nephrolithiasis. Genitourinary complications often occur in case of a severe longstanding disease and are associated with, the activity of bowel disease, especially in those who have undergone bowel surgery. As uncontrolled nephrolithiasis could impair renal function as well as adversely affect quality of life, proper monitoring, early detection, and prevention of the occurrence of urologic complications in CD is crucial. Few data are available about urolithiasis in patients with CD. Herein we report a case of a successful removal of a 2.7 cm calcium oxalate stone using percutaneous nephrolithotomy from a patient with long-standing CD with a previous surgery for small intestinal and colonic stricture.
Figure
-
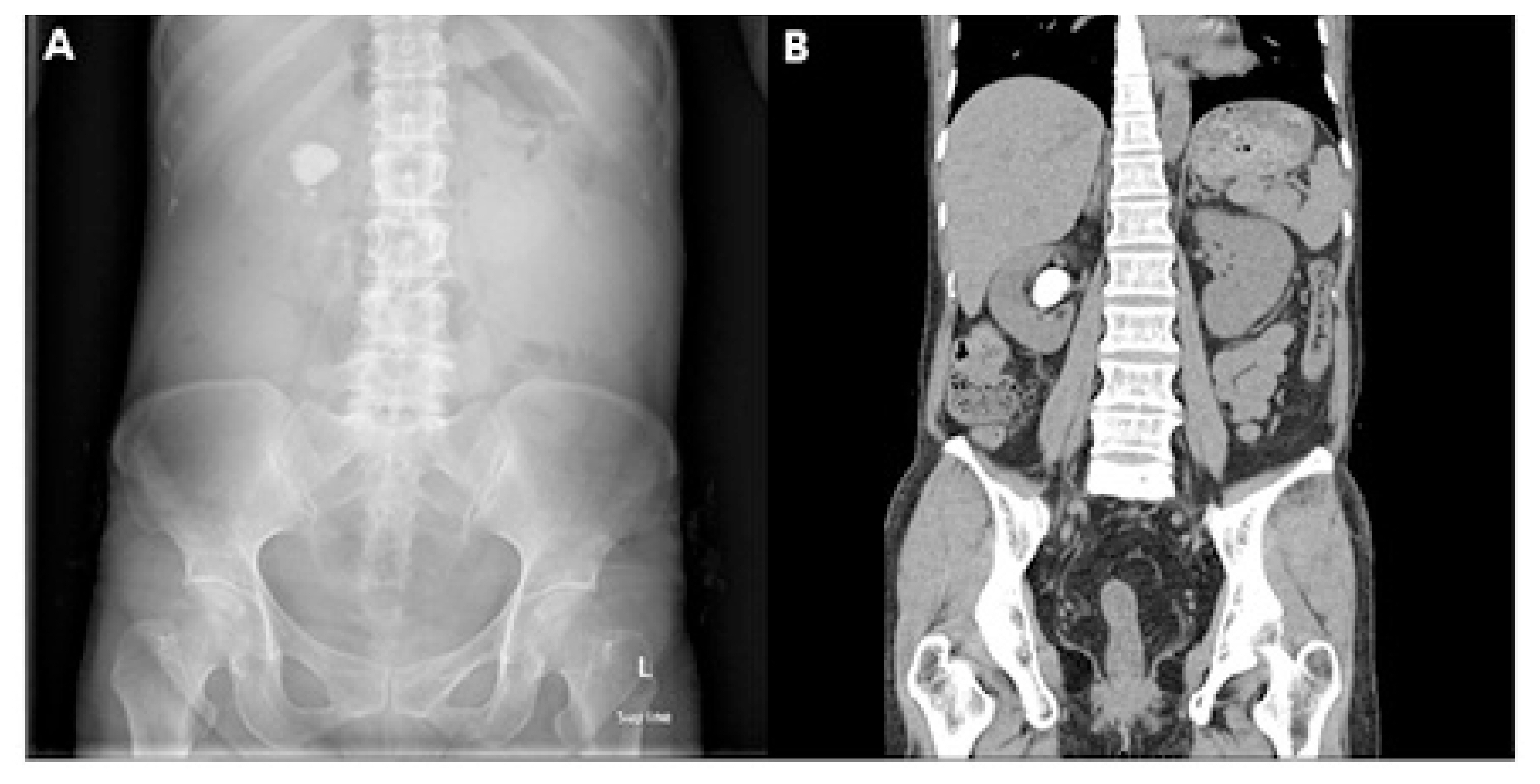
Fig. 1 Radiologic findings at the first visit. (A) X-ray of the abdomen at the first visit showing a 2.7 cm radio-opaque stone on the right upper quadrant. (B) Computed tomography of abdomen at the first visit showing right pelvicalyceal stone.
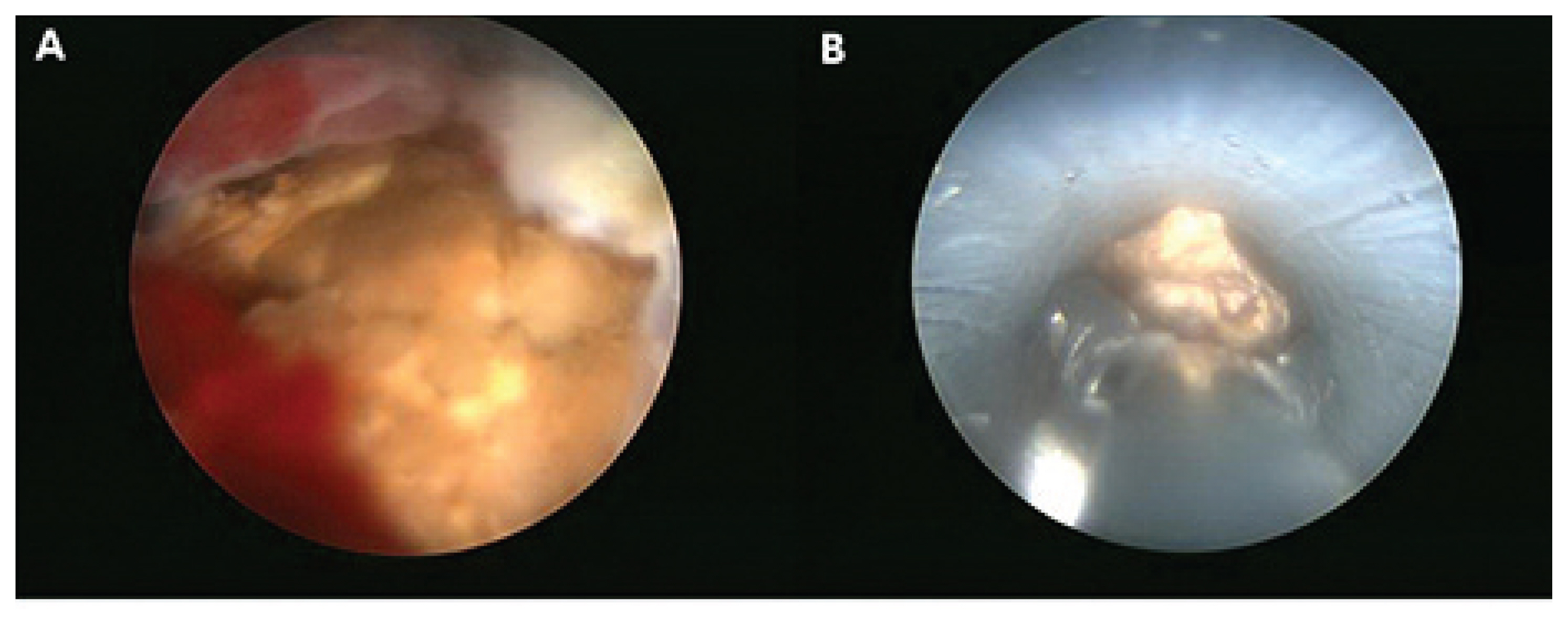
Fig. 2 Intra-operation findings of the stone. (A) Intra-operation finding of the stone. (B) Stone removal through percutaneous nephrotomy using forcep.
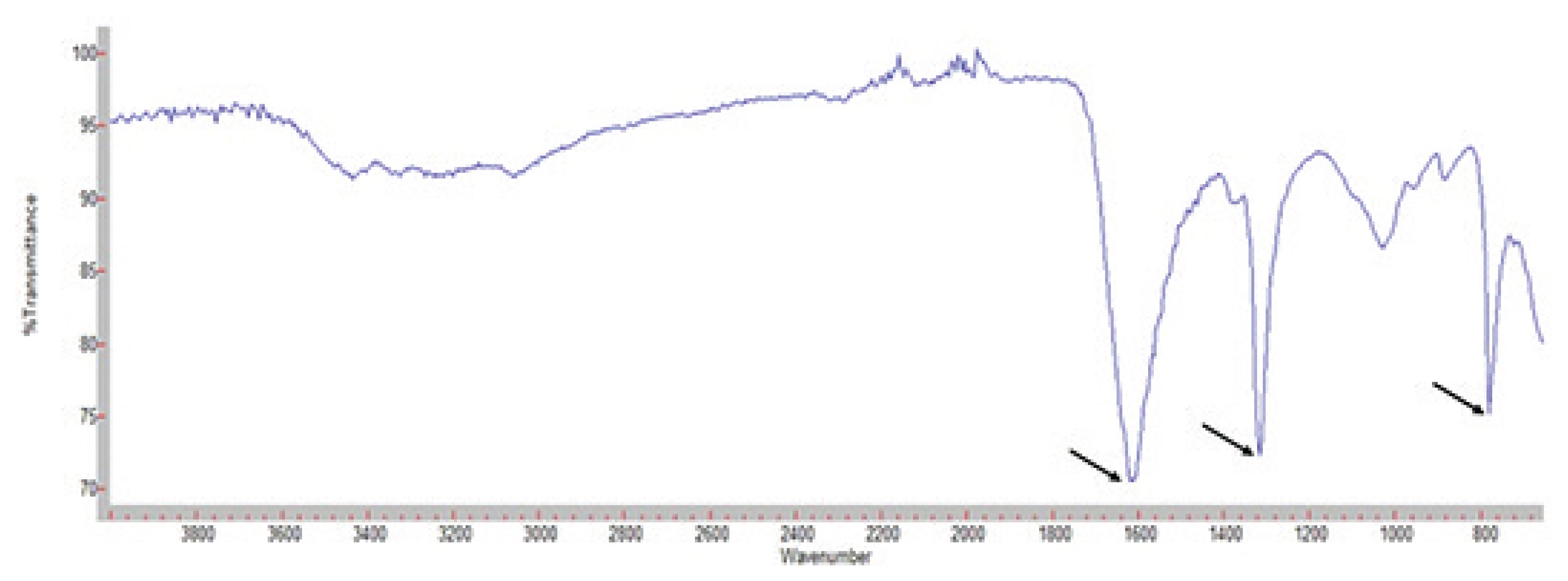
Fig. 3 Stone analysis using infrared spectroscopy shows peak at wavenumber of 1600, 1300, and 800 which means calcium oxalate stone. Nephrolithiasis in Crohn’s Disease
Reference
-
1. Gaspar SR, Mendonca T, Oliveira P, Oliveira T, Dias J, Lopes T. Urolithiasis and crohn’s disease. Urol Ann. 2016; 8:297–304.
Article2. Primas C, Novacek G, Schweiger K, Mayer A, Eser A, Papay P, et al. Renal insufficiency in IBD--prevalence and possible pathogenetic aspects. J Crohns Colitis. 2013; 7:e630–34.3. Ishii G, Nakajima K, Tanaka N, Hara H, Kato M, Ishii N. Clinical evaluation of urolithiasis in Crohn’s disease. Int J Urol. 2009; 16:477–80.
Article4. Mukewar S, Hall P, Lashner BA, Lopez R, Kiran RP, Shen B. Risk factors for nephrolithiasis in patients with ileal pouches. J Crohns Colitis. 2013; 7:70–8.
Article5. Pardi DS, Tremaine WJ, Sandborn WJ, Mc-Carthy JT. Renal and urologic complications of inflammatory bowel disease. Am J Gastroenterol. 1998; 93:504–14.
Article6. Corica D, Romano C. Renal Involvement in Inflammatory Bowel Diseases. J Crohns Colitis. 2016; 10:226–35.
Article7. Larsen S, Bendtzen K, Nielsen OH. Extraintestinal manifestations of inflammatory bowel disease: epidemiology, diagnosis, and management. Ann Med. 2010; 42:97–114.
Article8. Manganiotis AN, Banner MP, Malkowicz SB. Urologic complications of Crohn’s disease. Surg Clin North Am. 2001; 81:197–215. x
Article9. Gelzayd EA, Breuer RI, Kirsner JB. Nephrolithiasis in inflammatory bowel disease. Am J Dig Dis. 1968; 13:1027–34.
Article10. Nightingale JM, Lennard-Jones JE, Gertner DJ, Wood SR, Bartram CI. Colonic preservation reduces need for parenteral therapy, increases incidence of renal stones, but does not change high prevalence of gall stones in patients with a short bowel. Gut. 1992; 33:1493–7.
Article11. Coe FL, Parks JH, Asplin JR. The pathogenesis and treatment of kidney stones. N Engl J Med. 1992; 327:1141–52.
Article12. Earnest DL, Johnson G, Williams HE, Admirand WH. Hyperoxaluria in patients with ileal resection: an abnormality in dietary oxalate absorption. Gastroenterology. 1974; 66:1114–22.
Article13. Kumar R, Ghoshal UC, Singh G, Mittal RD. Infrequency of colonization with Oxalobacter formigenes in inflammatory bowel disease: possible role in renal stone formation. J Gastroenterol Hepatol. 2004; 19:1403–09.
Article14. Tiselius HG, Chaussy CG. Arguments for choosing extracorporeal shockwave lithotripsy for removal of urinary tract stones. Urolithiasis. 2015; 43:387–96.
Article15. Katsanos K, Tsianos E. The kidneys in inflammatory bowel disease. Annal Gastroenterology. 2007; 15:41–52.
