Acute Crit Care.
2021 Nov;36(4):286-293. 10.4266/acc.2021.00458.
Critical care management of pulmonary arterial hypertension in pregnancy: the pre-, peri- and post-partum stages
- Affiliations
-
- 1Division of Critical Care Medicine, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
- 2Excellence Center for Critical Care Medicine, King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand
- 3Division of Pulmonary and Critical Care Medicine, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
- 4Excellence Center for Sleep Disorder, King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand
- KMID: 2524310
- DOI: http://doi.org/10.4266/acc.2021.00458
Abstract
- The mortality rate of pulmonary hypertension in pregnancy is 25%–56%. Pulmonary arterial hypertension is the highest incidence among this group, especially in young women. Despite clear recommendation of pregnancy avoidance, certain groups of patients are initially diagnosed during the gestational age step into the third trimester. While the presence of right ventricular failure in early gestation is usually trivial, it can be more severe in the late trimester. Current evidence shows no consensus in the management and serious precautions for each stage of the pre-, peri- and post-partum periods of this specific group. Pulmonary hypertension-targeted drugs, mode of delivery, type of anesthesia, and some avoidances should be planned among a multidisciplinary team to enhance maternal and fetal survival opportunities. Sudden circulatory collapse from cardiac decompensation during the peri- and post-partum phases is detrimental, and mechanical support such as extracorporeal membrane oxygenation should be considered for mitigating hemodynamics and extending cardiac recovery time. Our review aims to explain the pathophysiology of pulmonary arterial hypertension and summarize the current evidence for critical management and precautions in each stage of pregnancy.
Keyword
Figure
-
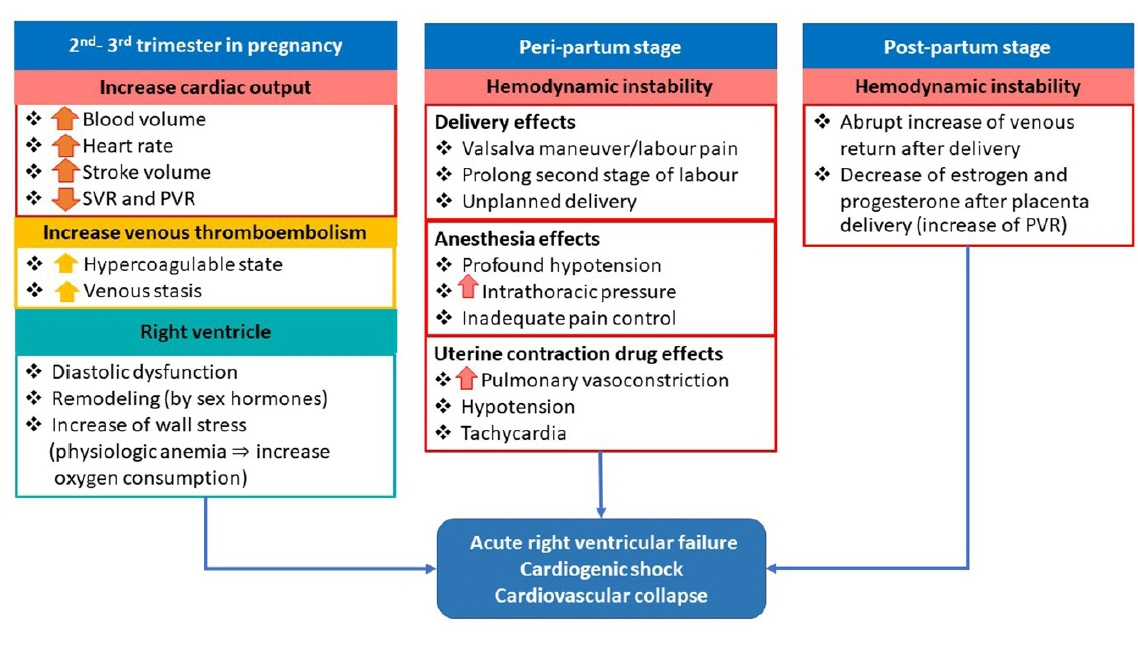
Figure 1. Pathophysiology of acute right ventricular failure, cardiogenic shock, and cardiovascular collapse in pregnant patients with pulmonary arterial hypertension during the pre-, peri- and post-partum stages. SVR: systemic vascular resistance; PVR: pulmonary vascular resistance.
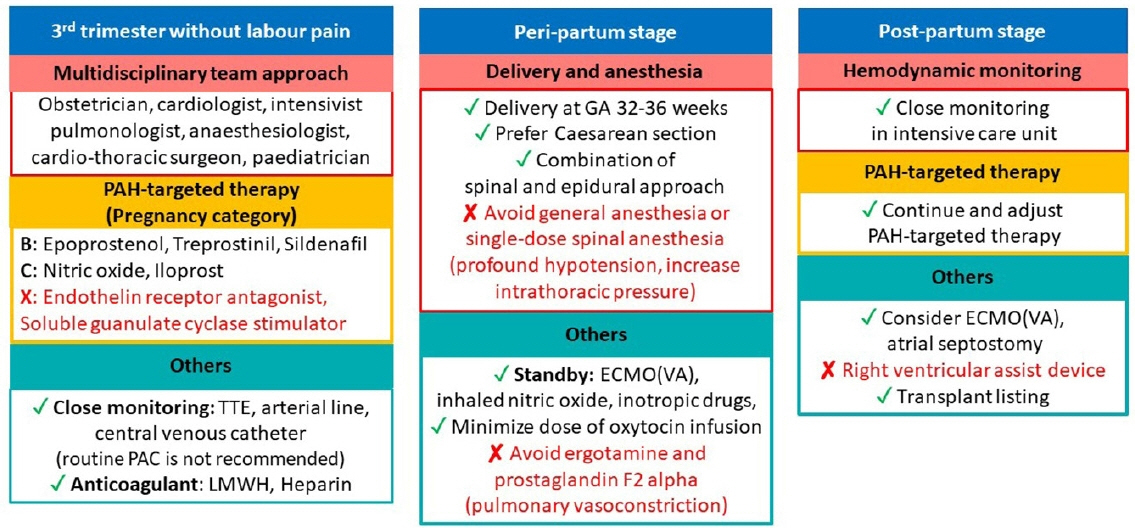
Figure 2. Critical care management for acute right ventricular failure, cardiogenic shock and cardiovascular collapse in pregnant patients with pulmonary arterial hypertension (PAH) during the pre-, peri- and post-partum stages. TTE: transthoracic echocardiography; LMWH: low molecular weight heparin; ECMO: extracorporeal membrane oxygenation; VA: veno-arterial.
Reference
-
1. Bédard E, Dimopoulos K, Gatzoulis MA. Has there been any progress made on pregnancy outcomes among women with pulmonary arterial hypertension? Eur Heart J. 2009; 30:256–65.2. Olsson KM, Jais X. Birth control and pregnancy management in pulmonary hypertension. Semin Respir Crit Care Med. 2013; 34:681–8.
Article3. Martínez MV, Rutherford JD. Pulmonary hypertension in pregnancy. Cardiol Rev. 2013; 21:167–73.
Article4. Roos-Hesselink J, Baris L, Johnson M, De Backer J, Otto C, Marelli A, et al. Pregnancy outcomes in women with cardiovascular disease: evolving trends over 10 years in the ESC Registry Of Pregnancy And Cardiac disease (ROPAC). Eur Heart J. 2019; 40:3848–55.
Article5. Yang M, Wang J, Zhang X, Zhuang Q, Wang R, Shen J, Lin J. Incidence and long-term outcomes of pregnant women complicated with pulmonary arterial hypertension during different pregnancies: a prospective cohort study from China. Int J Cardiol. 2021; 326:178–83.
Article6. Yang JZ, Fernandes TM, Kim NH, Poch DS, Kerr KM, Lombardi S, et al. Pregnancy and pulmonary arterial hypertension: a case series and literature review. Am J Obstet Gynecol MFM. 2021; 3:100358.
Article7. Sharma R, Kumar A, Aneja GK. Serial changes in pulmonary hemodynamics during pregnancy: a non-invasive study using doppler echocardiography. Cardiol Res. 2016; 7:25–31.
Article8. Madden BP. Pulmonary hypertension and pregnancy. Int J Obstet Anesth. 2009; 18:156–64.
Article9. Olsson KM, Channick R. Pregnancy in pulmonary arterial hypertension. Eur Respir Rev. 2016; 25:431–7.
Article10. Hall ME, George EM, Granger JP. The heart during pregnancy. Rev Esp Cardiol. 2011; 64:1045–50.
Article11. Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A. Physiological changes in pregnancy. Cardiovasc J Afr. 2016; 27:89–94.
Article12. Smith AM, Jones RD, Channer KS. The influence of sex hormones on pulmonary vascular reactivity: possible vasodilator therapies for the treatment of pulmonary hypertension. Curr Vasc Pharmacol. 2006; 4:9–15.
Article13. Christou HA, Khalil RA. Sex hormones and vascular protection in pulmonary arterial hypertension. J Cardiovasc Pharmacol. 2010; 56:471–4.
Article14. English KM, Jones RD, Jones TH, Morice AH, Channer KS. Gender differences in the vasomotor effects of different steroid hormones in rat pulmonary and coronary arteries. Horm Metab Res. 2001; 33:645–52.
Article15. Burt CC, Durbridge J. Management of cardiac disease in pregnancy. Contin Educ Anaesth Critic Care Pain. 2009; 9:44–7.
Article16. Neema PK. Eisenmenger syndrome: an unsolved malady. Ann Card Anaesth. 2012; 15:257–8.
Article17. Hsu CH, Gomberg-Maitland M, Glassner C, Chen JH. The management of pregnancy and pregnancy-related medical conditions in pulmonary arterial hypertension patients. Int J Clin Pract Suppl. 2011; (172):6–14.
Article18. Kumar A, Neema PK. Severe pulmonary hypertension and right ventricular failure. Indian J Anaesth. 2017; 61:753–9.
Article19. Bassily-Marcus AM, Yuan C, Oropello J, Manasia A, Kohli-Seth R, Benjamin E. Pulmonary hypertension in pregnancy: critical care management. Pulm Med. 2012; 2012:709407.
Article20. Huang S, DeSantis ER. Treatment of pulmonary arterial hypertension in pregnancy. Am J Health Syst Pharm. 2007; 64:1922–6.
Article21. Franchini M. Haemostasis and pregnancy. Thromb Haemost. 2006; 95:401–13.
Article22. Hellgren M. Hemostasis during normal pregnancy and puerperium. Semin Thromb Hemost. 2003; 29:125–30.
Article23. Szecsi PB, Jørgensen M, Klajnbard A, Andersen MR, Colov NP, Stender S. Haemostatic reference intervals in pregnancy. Thromb Haemost. 2010; 103:718–27.
Article24. Abid Memon H, Safdar Z, Goodarzi A. Use of extracorporeal membrane oxygenation in postpartum management of a patient with pulmonary arterial hypertension. Case Rep Pulmonol. 2018; 2018:7031731.
Article25. Ye J, Chen JY, Xu N, Wu B, Wang ZP, Xu HY, et al. Bilateral lung transplantation after caesarean section in pregnancy with severe pulmonary arterial hypertension: a case report. Medicine (Baltimore). 2019; 98:e18109.26. Ngatchou W, Ramadan AS, Van Nooten G, Antoine M. Left tilt position for easy extracorporeal membrane oxygenation cannula insertion in late pregnancy patients. Interact Cardiovasc Thorac Surg. 2012; 15:285–7.
Article27. Memon HA, Safdar Z. Use of extracorporeal membrane oxygenation in postpartum management of a patient with PAH. Chest. 2016; 150(4 Suppl):1220A.
Article28. Thorne S, MacGregor A, Nelson-Piercy C. Risks of contraception and pregnancy in heart disease. Heart. 2006; 92:1520–5.
Article29. Phoophiboon V, Jaimchariyatam N, Srimahachota S, Sirinawin C. Successful multimodality management of severe pulmonary arterial hypertension during pregnancy with VA-ECMO and atrial septostomy using stent. BMJ Case Rep. 2019; 12:e231916.
Article30. Rubin LJ. Primary pulmonary hypertension. Chest. 1993; 104:236–50.
Article31. Bonnin M, Mercier FJ, Sitbon O, Roger-Christoph S, Jaïs X, Humbert M, et al. Severe pulmonary hypertension during pregnancy: mode of delivery and anesthetic management of 15 consecutive cases. Anesthesiology. 2005; 102:1133–7.32. Monagle J, Manikappa S, Ingram B, Malkoutzis V. Pulmonary hypertension and pregnancy: the experience of a tertiary institution over 15 years. Ann Card Anaesth. 2015; 18:153–60.
Article33. Uebing A, Steer PJ, Yentis SM, Gatzoulis MA. Pregnancy and congenital heart disease. BMJ. 2006; 332:401–6.34. Liu S, Liston RM, Joseph KS, Heaman M, Sauve R, Kramer MS, et al. Maternal mortality and severe morbidity associated with low-risk planned cesarean delivery versus planned vaginal delivery at term. CMAJ. 2007; 176:455–60.
Article35. Hemnes AR, Kiely DG, Cockrill BA, Safdar Z, Wilson VJ, Al Hazmi M, et al. Statement on pregnancy in pulmonary hypertension from the Pulmonary Vascular Research Institute. Pulm Circ. 2015; 5:435–65.
Article36. Wong PS, Constantinides S, Kanellopoulos V, Kennedy CR, Watson D, Shiu MF. Primary pulmonary hypertension in pregnancy. J R Soc Med. 2001; 94:523–5.
Article37. Meng ML, Landau R, Viktorsdottir O, Banayan J, Grant T, Bateman B, et al. Pulmonary hypertension in pregnancy: a report of 49 cases at four tertiary North American sites. Obstet Gynecol. 2017; 129:511–20.38. Weeks SK, Smith JB. Obstetric anaesthesia in patients with primary pulmonary hypertension. Can J Anaesth. 1991; 38:814–6.
Article39. Martin JT, Tautz TJ, Antognini JF. Safety of regional anesthesia in Eisenmenger's syndrome. Reg Anesth Pain Med. 2002; 27:509–13.
Article40. McMillan E, Martin WL, Waugh J, Rushton I, Lewis M, Clutton-Brock T, et al. Management of pregnancy in women with pulmonary hypertension secondary to SLE and anti-phospholipid syndrome. Lupus. 2002; 11:392–8.41. Tamhane P, O'Sullivan G, Reynolds F. Oxytocin in parturients with cardiac disease. Int J Obstet Anesth. 2006; 15:332–3.
Article42. Weiss BM, Zemp L, Seifert B, Hess OM. Outcome of pulmonary vascular disease in pregnancy: a systematic overview from 1978 through 1996. J Am Coll Cardiol. 1998; 31:1650–7.
Article43. Agerstrand C, Abrams D, Biscotti M, Moroz L, Rosenzweig EB, D'Alton M, et al. Extracorporeal membrane oxygenation for cardiopulmonary failure during pregnancy and postpartum. Ann Thorac Surg. 2016; 102:774–9.44. Parissis JT, Paraskevaidis I, Bistola V, Farmakis D, Panou F, Kourea K, et al. Effects of levosimendan on right ventricular function in patients with advanced heart failure. Am J Cardiol. 2006; 98:1489–92.
Article45. Kerbaul F, Rondelet B, Motte S, Fesler P, Hubloue I, Ewalenko P, et al. Effects of norepinephrine and dobutamine on pressure load-induced right ventricular failure. Crit Care Med. 2004; 32:1035–40.
Article46. Eichhorn EJ, Konstam MA, Weiland DS, Roberts DJ, Martin TT, Stransky NB, et al. Differential effects of milrinone and dobutamine on right ventricular preload, afterload and systolic performance in congestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol. 1987; 60:1329–33.
Article47. Cheung PY, Barrington KJ. The effects of dopamine and epinephrine on hemodynamics and oxygen metabolism in hypoxic anesthetized piglets. Crit Care. 2001; 5:158–66.48. Schreuder WO, Schneider AJ, Groeneveld AB, Thijs LG. Effect of dopamine vs norepinephrine on hemodynamics in septic shock: emphasis on right ventricular performance. Chest. 1989; 95:1282–8.49. Kim H, Cho YH. Role of extracorporeal cardiopulmonary resuscitation in adults. Acute Crit Care. 2020; 35:1–9.
Article50. Ko RE, Chung CR, Yang JH, Jeon K, Suh GY, Oh SY, et al. Use of extracorporeal membrane oxygenation in postpartum patients with refractory shock or respiratory failure. Sci Rep. 2021; 11:887.
Article51. Moore SA, Dietl CA, Coleman DM. Extracorporeal life support during pregnancy. J Thorac Cardiovasc Surg. 2016; 151:1154–60.
Article52. Humbert M, Sitbon O, Simonneau G. Treatment of pulmonary arterial hypertension. N Engl J Med. 2004; 351:1425–36.
Article53. Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016; 37:67–119.54. Famuyide AO, Hopkins MR, El-Nashar SA, Creedon DJ, Vasdev GM, Driscoll DJ, et al. Hysteroscopic sterilization in women with severe cardiac disease: experience at a tertiary center. Mayo Clin Proc. 2008; 83:431–8.
Article
