Treatment of a Huge Aneurysmal Bone Cyst of the Talus through a Segmental Bone Graft of the Tricortical Bone: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Kangdong Sacred Heart Hospital, Seoul, Korea
- KMID: 2523301
- DOI: http://doi.org/10.14193/jkfas.2021.25.4.185
Abstract
- An aneurysmal bone cyst (ABC) can occur in many parts of the human body, but a primary ABC of the talus is extremely rare. ABCs are benign, but aggressively growing tumors that usually occur in the first two decades of life. Patients mainly complain of pain, limited movement of the involved joint or a palpable mass. Pain may worsen suddenly because of pathological fractures. If not treated properly, ABC has a risk of local recurrence, followed by the destruction of the joint and a significant functional deficit. While the complete removal of the bone tumor is essential, it is also important to treat the resultant bone defect after removal. The talus has an important part to play in weight-bearing. Therefore, an appropriate bone graft is required for large bone defects that occur after an ABC removal from the talus. We report a primary ABC of the talus in a 28-year-old male that was treated by curettage and a bone pillar pattern graft of autologous tricortical iliac crest bone. The patient had an excellent functional outcome with early weight-bearing, and there was no recurrence at 16 months of follow-up.
Keyword
Figure
-

Figure. 1 (A~C) Radiolucent oval cystic lesions on the lateral body of the talus with reactive sclerotic borders on preoperative ankle radiographs.

Figure. 2 On the preoperative magnetic resonance imaging, the T1 image shows a well-delineated low-signal intensity lesion (A, B). The T2 image shows the high-signal intensity image (C, D). Multiple fluid lines and peripheral edema of the talus body without breakage or soft tissue expansion are observed.
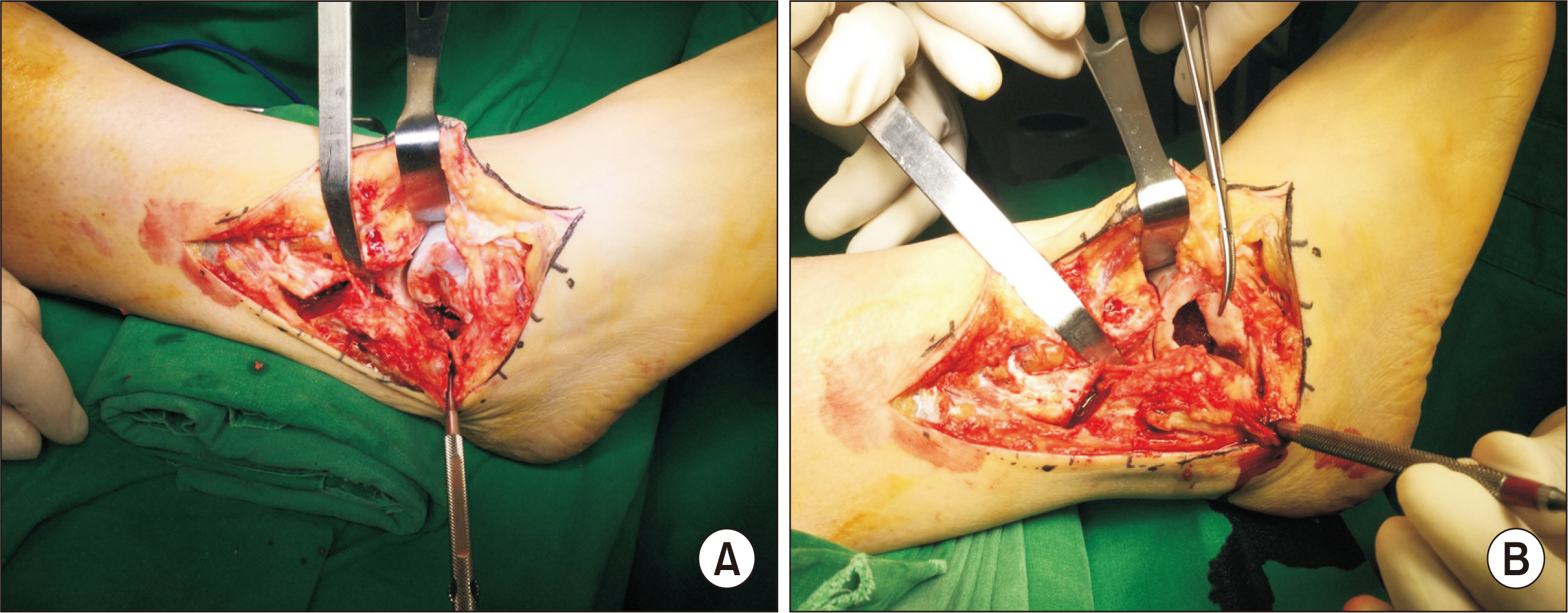
Figure. 3 (A) Distal fibular osteotomy was performed to access the lateral talar wall. (B) A window was created on the lateral talar wall by mess.

Figure. 4 Autologous bone in the form of tricortical bone was harvested from the iliac crest.

Figure. 5 Tricortical bone was divided and molded into 2.5 cm high cuboid-shaped pillars and bone pillars were implanted through a window by turning them standing up and down without any gaps in the bone defect.
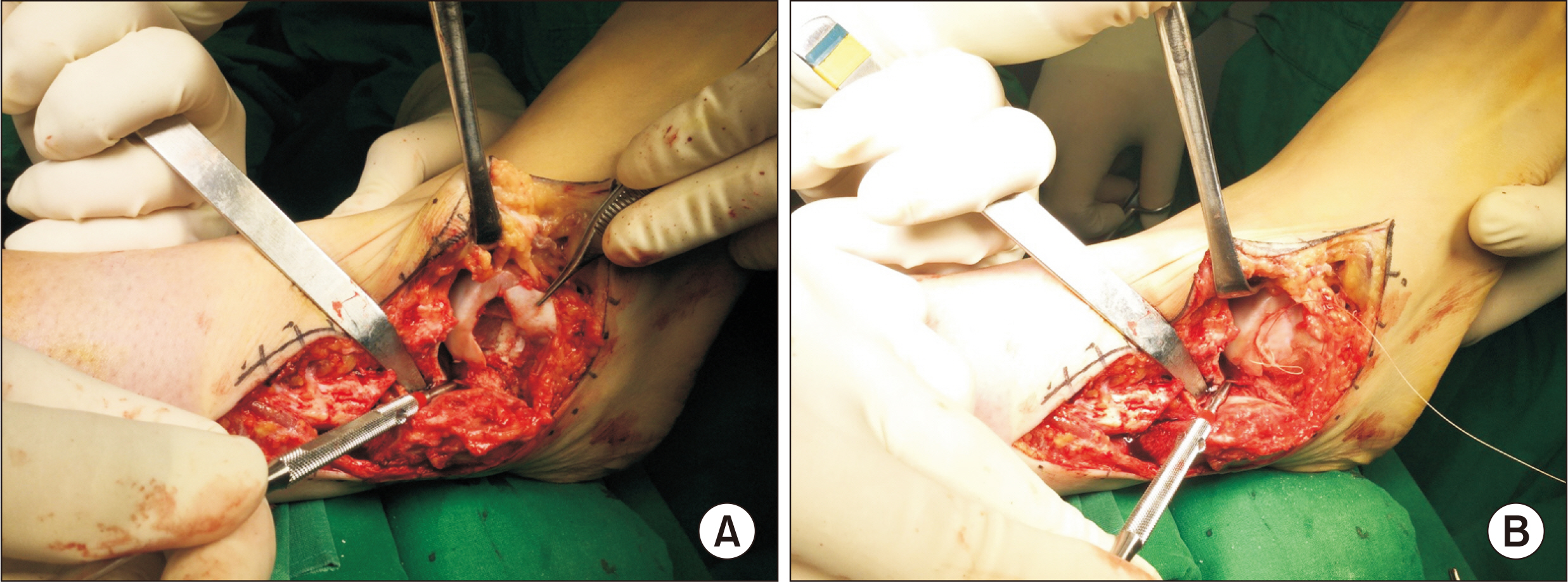
Figure. 6 Bone graft was done with autologous iliac bone columns and allogenic bone (A) and window was repaired with absorbable suture (B).

Figure. 7 On medium magnititude power, microscopic finding shows basically thin various cystic septa structures. These septa are composed of loosely arranged spindle cells, benign multinucleated giant cells and some inflammatory cells. Also, there is no atypia at spindle cells (H&E, x200) (A). Microscopic finding shows predominantly solid area, at which spindle cell proliferation and several giant cells are prominent. Also, there are some foci of reactive new bone formation (H&E, x200) (B).
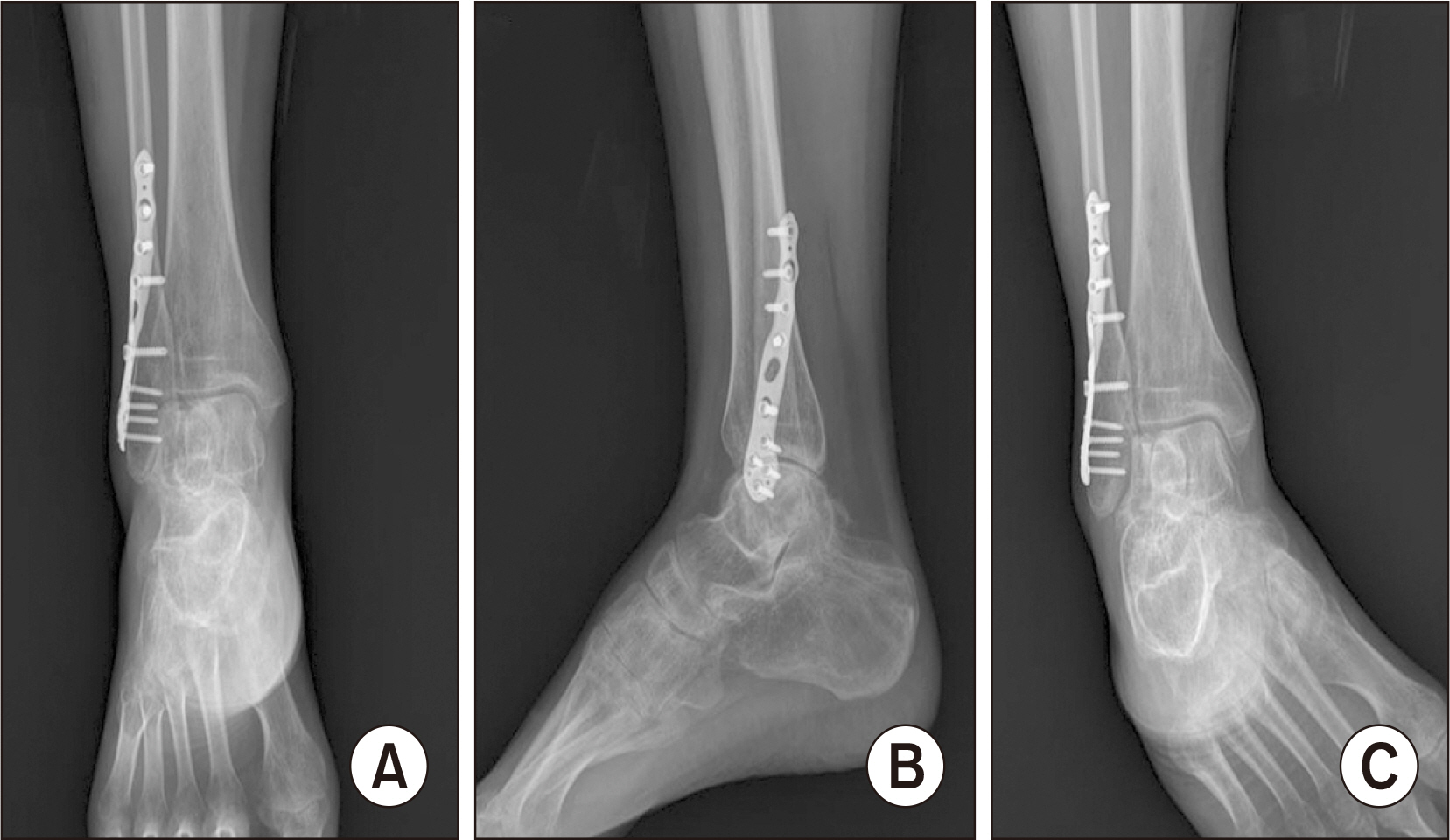
Figure. 8 (A~C) On the postoperative 15 months ankle radiographs show bone union of the distal fibula osteotomy site. Ankle joint and talar height were maintained without cortical bone fracture or damage of the articular surface.
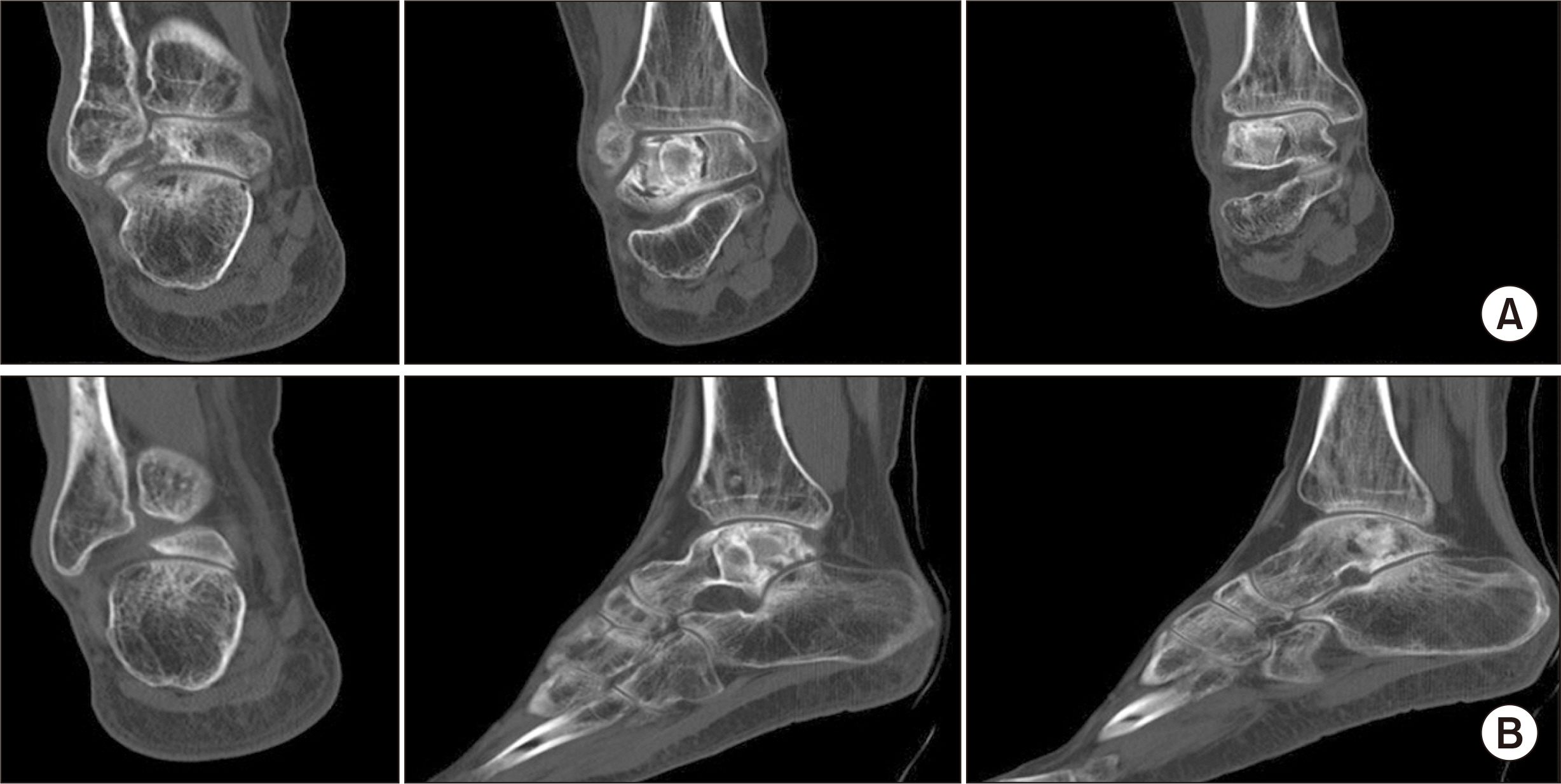
Figure. 9 (A, B) After surgery for metal remove, computerized tomography scan shows no evidence of talar dome collapse. Proper bone union was achieved at the site of autologous bone graft and distal fibular osteotomy, there were no recurrent lesions.
Reference
-
References
1. Cybulski GR, Anson J, Gleason T, Homsi MF, Reyes MG. 1989; Aneurysmal bone cyst of the thoracic spine: treatment by excision and segmental stabilization with Luque rods. Neurosurgery. 24:273–6. doi: 10.1227/00006123-198902000-00020. DOI: 10.1227/00006123-198902000-00020. PMID: 2918979.
Article2. Jaffe HL. 1950; Aneurysmal bone cyst. Bull Hosp Joint Dis. 11:3–13. PMID: 14783698.3. Mankin HJ, Hornicek FJ, Ortiz-Cruz E, Villafuerte J, Gebhardt MC. 2005; Aneurysmal bone cyst: a review of 150 patients. J Clin Oncol. 23:6756–62. doi: 10.1200/JCO.2005.15.255. DOI: 10.1200/JCO.2005.15.255. PMID: 16170183.
Article4. Lichtenstein L. 1950; Aneurysmal bone cyst. A pathological entity commonly mistaken for giant-cell tumor and occasionally for hemangioma and osteogenic sarcoma. Cancer. 3:279–89. doi: 10.1002/1097-0142(1950)3:2<279::AID-CNCR2820030209>3.0.CO;2-F. DOI: 10.1002/1097-0142(1950)3:2<279::AID-CNCR2820030209>3.0.CO;2-F.5. Silverberg SG, DeLellis RA, Frable WJ. 1997. Principles and practice of surgical pathology and cytopathology. 3rd ed. Churchill Livingstone;New York:6. Park JS, Suh JS, Choi JY. 2019; Chondroblastoma of the talus mimicking an aneurysmal bone cyst: a case report. J Korean Foot Ankle Soc. 23:31–4. doi: 10.14193/jkfas.2019.23.1.31. DOI: 10.14193/jkfas.2019.23.1.31.
Article7. Rosai J. 2004. Rosai and Ackerman's surgical pathology. 9th ed. Mosby;Edinburgh:8. Dhillon MS, Singh B, Gill SS, Walker R, Nagi ON. 1993; Management of giant cell tumor of the tarsal bones: a report of nine cases and a review of the literature. Foot Ankle. 14:265–72. doi: 10.1177/107110079301400506. DOI: 10.1177/107110079301400506. PMID: 8349212.
Article9. Luna AR, Fahandez-Saddi H, Garcia AV, Reina Cde J, Martin JV. 2004; Aneurysmal bone cyst in children involving infrequent locations. Report on two cases. Chir Organi Mov. 89:347–52. PMID: 16048058.10. Sharma S, Gupta P, Sharma S, Singh M, Singh D. 2012; Primary aneurysmal bone cyst of talus. J Res Med Sci. 17:1192–4. PMID: 23853640. PMCID: PMC3703174.11. Manjunatha V, Thimmegowda RB. 2016; Aneurysmal bone cyst of talus- a case report. In J Sci Res Rev. 5:52–9.
