Outcomes of Dilation of Recalcitrant Pancreatic Strictures Using a Wire-Guided Cystotome
- Affiliations
-
- 1Department of Gastroenterology, Seth GS Medical College and King Edward Memorial Hospital, Mumbai, India
- KMID: 2522712
- DOI: http://doi.org/10.5946/ce.2020.297
Abstract
- Background/Aims
Pancreatic strictures in chronic pancreatitis are treated using endoscopic retrograde cholangiopancreatography (ERCP) with plastic stent placement. The management of recalcitrant strictures remains a challenge, with the use of a Soehendra stent retriever or a needle knife described in case reports. Here, we discuss our experience with dilation of dominant pancreatic strictures with a 6-Fr cystotome.
Methods
A retrospective review of an endoscopy database was performed to search for patients with pancreatic strictures recalcitrant to conventional methods of dilation in which a cystotome was used. Technical success was defined as the successful dilation of the stricture with plastic stent placement. Functional success was defined as substantial pain relief or resolution of pancreatic fistulae.
Results
Ten patients (mean age, 30.8 years) underwent dilation of a dominant pancreatic stricture secondary to chronic pancreatitis, with a 6-Fr cystotome. Seven patients presented with pain. Three patients had pancreatic fistulae (two had pancreatic ascites and one had a pancreaticopleural fistula). The median stricture length was 10 mm (range, 5–25 mm). The head of the pancreas was the most common location of the stricture (60%). Technical and functional success was achieved in all patients. One patient had self-limiting bleeding, whereas another patient developed mild post-ERCP pancreatitis.
Conclusions
The use of a 6-Fr cystotome (diathermy catheter) can be an alternative method for dilation of recalcitrant pancreatic strictures after the failure of conventional modalities.
Figure
-
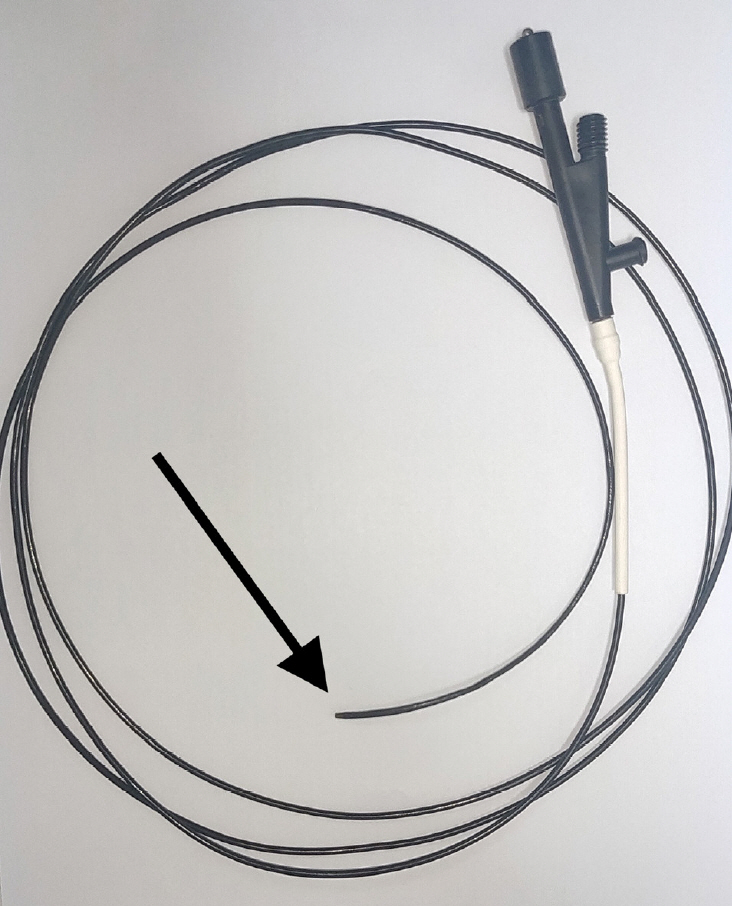
Fig. 1. A 6-Fr monopolar cystotome used for dilation. The arrow points to the metal tip.

Fig. 2. (A) Stricture at the neck of the pancreas (black arrow) with abnormal pancreaticobiliary ductal union Komi type IIA with a long common channel (red arrow), with the cystotome in the region of the head. (B) Cystotome passed across the stricture (arrow), with evident drainage of contrast. (C) Stent placed with complete drainage of contrast.

Fig. 3. Stricture in region of the head (black arrow) with leak from the tail of the pancreas (red arrow) leading to a pancreaticopleural fistula.
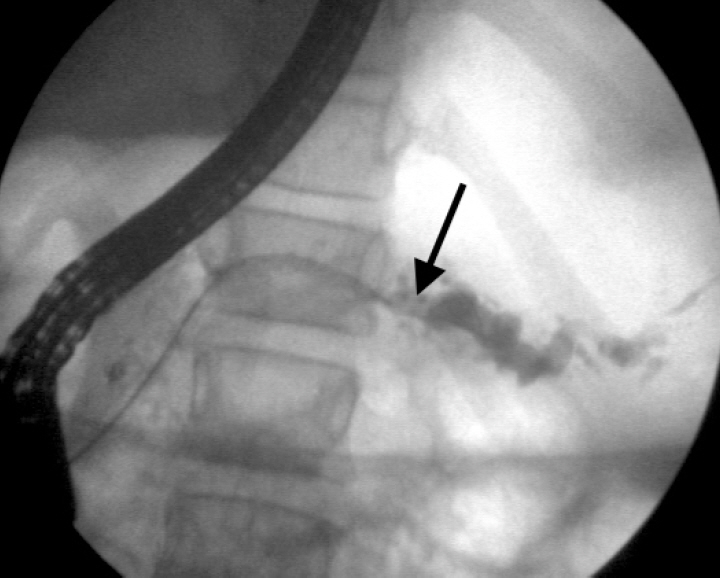
Fig. 4. Stricture in the proximal body of the pancreas (arrow) with a distally dilated pancreatic duct.

Fig. 5. Algorithm proposal for dilation of dominant pancreatic strictures. ERCP, endoscopic retrograde cholangiopancreatography; MRCP, magnetic resonance cholangiopancreatography.
Reference
-
1. Godil A, Chen YK. Endoscopic management of benign pancreatic disease. Pancreas. 2000; 20:1–13.
Article2. Tandan M, Reddy DN, Santosh D, et al. Extracorporeal shock wave lithotripsy and endotherapy for pancreatic calculi-a large single center experience. Indian J Gastroenterol. 2010; 29:143–148.
Article3. Delhaye M, Matos C, Devière J. Endoscopic management of chronic pancreatitis. Gastrointest Endosc Clin N Am. 2003; 13:717–742.
Article4. Dumonceau JM, Delhaye M, Tringali A, et al. Endoscopic treatment of chronic pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) guideline - updated August 2018. Endoscopy. 2019; 51:179–193.
Article5. Seicean A, Vultur S. Endoscopic therapy in chronic pancreatitis: current perspectives. Clin Exp Gastroenterol. 2015; 8:1–11.
Article6. Jafri M, Sachdev A, Sadiq J, et al. Efficacy of endotherapy in the treatment of pain associated with chronic pancreatitis: a systematic review and meta-analysis. JOP. 2017; 18:125–132.7. Saftoiu A, Vilmann A, Vilmann P. Endoscopic ultrasound-guided drainage of pancreatic pseudocysts. Endosc Ultrasound. 2015; 4:319–323.
Article8. Kim E, Aouattah T, Deprez PH. Successful retrograde and antegrade passage of narrow and complete pancreatic strictures using a cystogastrostome. Endoscopy. 2011; 43(Suppl 2):E340–E341.
Article9. Tringali A, Bove V, Vadalà di Prampero SF, et al. Long-term follow-up after multiple plastic stenting for refractory pancreatic duct strictures in chronic pancreatitis. Endoscopy. 2019; 51:930–935.
Article10. Faigel DO, Ginsberg GG, Kochman ML. Innovative use of the Soehendra stent retriever for biliary stricture recannalization. Gastrointest Endosc. 1996; 44:635.
Article11. Baron TH, Morgan DE. Dilation of a difficult benign pancreatic duct stricture using the Soehendra stent extractor. Gastrointest Endosc. 1997; 46:178–180.
Article12. Kawamoto H, Ishida E, Ogawa T, et al. Dissection of a refractory pancreatic-duct stricture by using a pre-cutting needle-knife. Gastrointest Endosc. 2006; 63:190–192.
Article13. Itoi T, Sofuni A, Itokawa F, et al. Transpapillary incision of refractory circumscript pancreatic duct stricture using wire-guided snare forceps. World J Gastroenterol. 2010; 16:1541–1544.
Article14. Kawakami H, Kuwatani M, Kawakubo K, et al. Transpapillary dilation of refractory severe biliary stricture or main pancreatic duct by using a wire-guided diathermic dilator (with video). Gastrointest Endosc. 2014; 79:338–343.
Article15. Puri R, Bhatia S, Bansal RK, Sud R. Endoscopic management of difficult benign biliary and pancreatic strictures using a wire-guided cystotome: experience with 25 cases. Endosc Int Open. 2018; 6:E797–E800.
Article16. Farnbacher MJ, Mühldorfer S, Wehler M, Fischer B, Hahn EG, Schneider HT. Interventional endoscopic therapy in chronic pancreatitis including temporary stenting: a definitive treatment? Scand J Gastroenterol. 2006; 41:111–117.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Difficult Pancreatic Duct Strictures Using a Cystotome: A Single-Center Experience
- Use of a Cutting Balloon Dilation as a Rescue Therapy in Patients with Benign Bilioenteric Anastomotic Strictures Refractory to Conventional Balloon Dilation
- Dilatation of Severe Corrosive Esophageal Stricture Guided by Right Coronary Artery Catheter
- Endoscopic Balloon Dilation for Crohn’s Disease-Associated Strictures
- Technical tips for endoscopic ultrasound-guided pancreatic duct access and drainage
