Contralateral Interhemispheric Transcallosal Approach for Thalamic Cystic Cavernous Malformation
- Affiliations
-
- 1Department of Neurosurgery, Pusan National University Hospital, Pusan National University College of Medicine, Busan, Korea
- KMID: 2522225
- DOI: http://doi.org/10.14791/btrt.2021.9.e15
Abstract
- A 42-year-old man presented with a headache and right hemiparesis and was found to have a cystic mass with a calcified mural nodule in the left thalamus. Because the thalamus is surrounded by vital neurovascular structures, the surgical approach to thalamic lesions can be challenging. We decided to remove the mass for decompression and pathological diagnosis. The mass was removed through a contralateral interhemispheric transcallosal transchoroidal approach with less retraction and parenchymal injury than other approaches to avoid brain retraction and cortical injury. The pathological diagnosis was cavernous malformation. Temporary worsening of the preoperative hemiparesis was recovered over two months following surgery. Tolerable thalamic pain syndrome remained. Here, we report a rare case of thalamic cavernous malformation with a favorable outcome through a contralateral surgical approach.
Keyword
Figure
-

Fig. 1 Preoperative radiologic findings. A: CT scanning shows a cystic mass with peripheral calcified nodule at left thalamus and hydrocephalus. B: T2-weighted MR axial image shows a lobulated cyst with fluid-fluid level and obstructive hydrocephalus. C: T1-weighted MR axial image shows a lobulated cyst with peripheral high signal mass. D: T1-weighted enhanced MR axial image shows subtle enhanced cystic mass at left thalamus.

Fig. 2 Postoperative radiologic findings. A: Surgical trajectory of contralateral interhemispheric transcallosal approach (red arrows) on T2-weighted MR coronal image. B: Postoperative CT coronal image shows contralateral callosotomy and ventricular catheter through the surgical route. C and D: Postoperative follow-up MRI shows removal of solid component and disappearance of mass effect without any neurovascular injury.
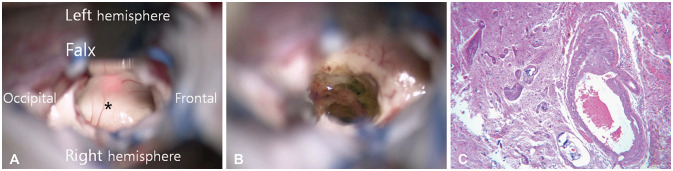
Fig. 3 Operative and pathologic findings. A: The floor of left lateral ventricle (asterisk) was upward displaced by thalamic mass. B: Gliosis and hemosiderin deposits are seen along the margin of cavernous malformation. C: Microscopic finding shows some abnormal shaped vessels that are consistent with cavernous malformation (hematoxylin & eosin, ×100).
Reference
-
1. Sarris CE, Atwal GS, Nakaji P. Thalamic cavernous malformations. Handb Clin Neurol. 2017; 143:297–302. PMID: 28552153.2. Cinalli G, Aguirre DT, Mirone G, et al. Surgical treatment of thalamic tumors in children. J Neurosurg Pediatr. 2018; 03. 21:247–257. PMID: 29271729.3. Kumar A, Sharma R, Garg A, Sharma BS. Contralateral anterior interhemispheric transparaterminal gyrus approach for thalamopeduncular pilocytic astrocytoma in an adult: technical report. World Neurosurg. 2016; 87:21–25. PMID: 26409092.4. Zaidi HA, Chowdhry SA, Nakaji P, Abla AA, Spetzler RF. Contralateral interhemispheric approach to deep-seated cavernous malformations: surgical considerations and clinical outcomes in 31 consecutive cases. Neurosurgery. 2014; 75:80–86. PMID: 24618803.5. Rangel-Castilla L, Spetzler RF. The 6 thalamic regions: surgical approaches to thalamic cavernous malformations, operative results, and clinical outcomes. J Neurosurg. 2015; 123:676–685. PMID: 26024002.6. Schwartz C, Grillhösl A, Schichor C, et al. Symptomatic cavernous malformations of the brainstem: functional outcome after microsurgical resection. J Neurol. 2013; 260:2815–2822. PMID: 23974645.7. Otani N, Fujioka M, Oracioglu B, et al. Thalamic cavernous angioma: paraculminar supracerebellar infratentorial transtentorial approach for the safe and complete surgical removal. Acta Neurochir Suppl. 2008; 103:29–36. PMID: 18496942.8. Lanzino G, Wanebo JE, Spetzler RF. Contralateral interhemispheric resection of thalamic cavernous malformations with frameless stereotaxy. Operat Tech Neurosurg. 2002; 5:191–197.9. Mathiesen T, Edner G, Kihlström L. Deep and brainstem cavernomas: a consecutive 8-year series. J Neurosurg. 2003; 99:31–37. PMID: 12854740.10. Li D, Zhang J, Hao S, et al. Surgical treatment and long-term outcomes of thalamic cavernous malformations. World Neurosurg. 2013; 79:704–713. PMID: 22381871.11. Pandey P, Westbroek EM, Gooderham PA, Steinberg GK. Cavernous malformation of brainstem, thalamus, and basal ganglia: a series of 176 patients. Neurosurgery. 2013; 72:573–589. discussion 588–9. PMID: 23262564.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Giant Cystic Cerebral Cavernous Malformation with Multiple Calcification: Case Report
- Surgical Approaches to Paraclinoid Aneurysms
- Surgical Approaches for Symptomatic Cerebral Cavernous Malformations of the Thalamus and Brainstem
- Surgical Treatment of Cavernous Malformation of Pineal Region
- A Case of Orbital Cavernous Angioma Associated with Intracranial Venous Anomalies
