Modified Orbitozygomatic Approach for Resecting a Parasellar Tumor in a Single Institution
- Affiliations
-
- 1Department of Neurosurgery, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2522220
- DOI: http://doi.org/10.14791/btrt.2021.9.e24
Abstract
- Background
Modified orbitozygomatic craniotomy is characterized by simplicity and wide exposure. The purpose of the present study was to describe a modified orbitozygomatic approach without resecting the zygomatic arch for large parasellar tumor surgeries.
Methods
Between April 2016 and December 2019, seven patients with parasellar tumor underwent surgiest with a modified orbitozygomatic approach. Surgical procedures, clinical outcomes, and complications were analyzed.
Results
This study included 3 meningiomas, 2 pituitary adenomas, 1 chondrosarcoma, and 1 schwannoma. Modified orbitozygomatic craniotomy provides a wider surgical freedom in the opticocarotid and prechiasmatic cistern than frontotemporal craniotomy without orbitotomy, Total, subtotal, and partial resections were achieved for 3, 2, and 2 patients, respectively. Reasons for partial resections were tight adhesion to the carotid artery and encasing of the carotid artery. Permanent morbidities developed in one patient with 3rd nerve palsy and one patient with hemiparesis.
Conclusion
Modified orbitozygomatic approach can provide the shortest access to the interpeduncular cistern with a minimum brain retraction. Surgeons who experience surgical challenge during the conventional approach for parasellar tumor resection are recommended to learn the modified orbitozygomatic approach.
Keyword
Figure
-
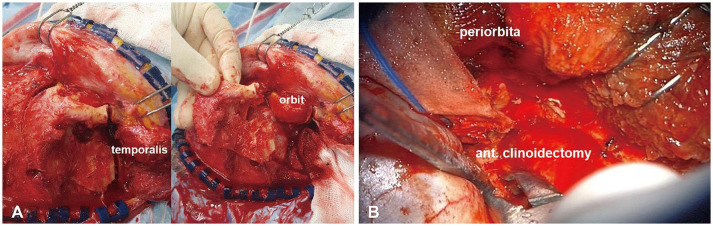
Fig. 1 One-piece frontotemporal craniotomy accompanied by orbitotomy following reflection of the temporalis muscle. A: Orbit is exposed after a modified orbitozygomatic craniotomy. B: Parasellar regions are approached by anterior clinoidectomy.
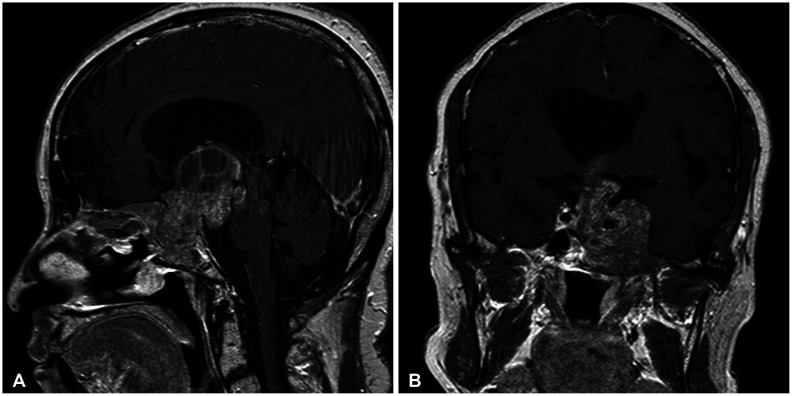
Fig. 2 Preoperative sagittal (A) and coronal (B) T1-enhanced images. Large pituitary adenoma (3.5×5.8×6.3 cm) noted in sellar, suprasellar, the third ventricle, and the left cavernous sinus with an upward displacement of the optic chiasm and an encasement of the left internal carotid artery.
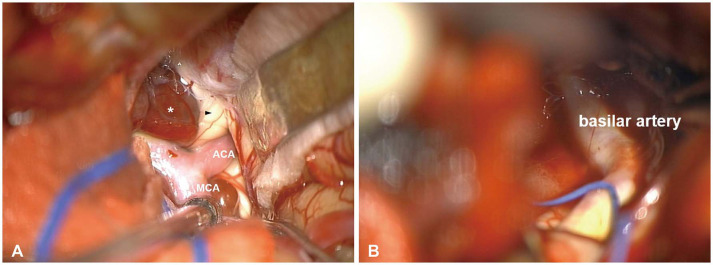
Fig. 3 Intraoperative findings. A: Left optic nerve (arrowhead) compressed by a tumor (asterisk). B: After the tumor’s removal, basilar artery is noted. ACA, anterior cerebral artery; MCA, middle cerebral artery.

Fig. 4 Postoperative MR images. A: Axial T1-enhanced image showing removal of the lesion located in sellar, suprasellar, and the third ventricle. B: Coronal T1-enhanced image shows that hydrocephalus is resolved but remnant tumor is noted in the left cavernous sinus.
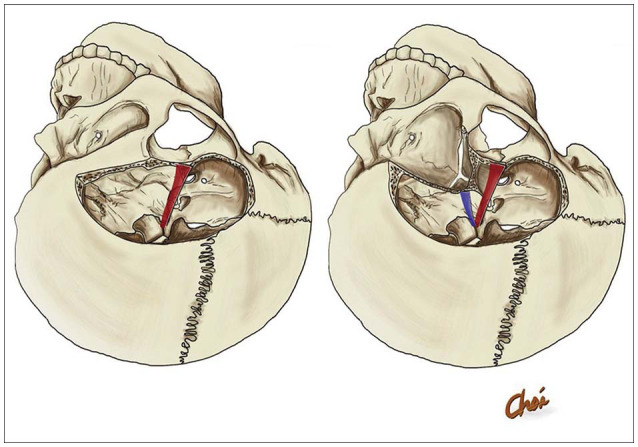
Fig. 5 Illustrated comparison of pterional approach (red) and modified orbitozygomatic approach (blue).
Reference
-
1. Jane JA, Park TS, Pobereskin LH, Winn HR, Butler AB. The supraorbital approach: technical note. Neurosurgery. 1982; 11:537–542. PMID: 7145070.2. Andaluz N, Van Loveren HR, Keller JT, Zuccarello M. Anatomic and clinical study of the orbitopterional approach to anterior communicating artery aneurysms. Neurosurgery. 2003; 52:1140–1148. discussion 1148-9. PMID: 12699559.3. Fujitsu K, Kuwabara T. Orbitocraniobasal approach for anterior communicating artery aneurysms. Neurosurgery. 1986; 18:367–369. PMID: 3517674.4. Smith RR, Al-Mefty O, Middleton TH. An orbitocranial approach to complex aneurysms of the anterior circulation. Neurosurgery. 1989; 24:385–391. PMID: 2927612.5. Balasingam V, Noguchi A, McMenomey SO, Delashaw JB Jr. Modified osteoplastic orbitozygomatic craniotomy. Technical note. J Neurosurg. 2005; 102:940–944. PMID: 15926727.6. Tanriover N, Ulm AJ, Rhoton AL Jr, Kawashima M, Yoshioka N, Lewis SB. One-piece versus two-piece orbitozygomatic craniotomy: quantitative and qualitative considerations. Neurosurgery. 2006; 58:ONS-229–ONS-237. discussion ONS-237.7. Cheng CM, Chang CF, Ma HI, Chiang YH, McMenomey SO, Delashaw JB Jr. Modified orbitozygomatic craniotomy for large medial sphenoid wing meningiomas. J Clin Neurosci. 2009; 16:1157–1160. PMID: 19560361.8. López-Elizalde R, Robledo-Moreno E, O Shea-Cuevas G, Matute-Villaseñor E, Campero Á, Godínez-Rubí M. Modified orbitozygomatic approach without orbital roof removal for middle fossa lesions. J Korean Neurosurg Soc. 2018; 61:407–414. PMID: 29631381.9. Cherekaev VA, Gol'bin DA, Belov AI, Radchenkov NS, Lasunin NV, Vinokurov AG. Orbitozygomatic approaches to the skull base. Zh Vopr Neirokhir Im N N Burdenko. 2015; 79:95–101. PMID: 26529627.10. Kim IS, Rha HK, Lee KJ, et al. Surgical approaches to the middle cranial base tumors. J Korean Neurosurg Soc. 2001; 30:1079–1085.11. Schwartz MS, Anderson GJ, Horgan MA, Kellogg JX, McMenomey SO, Delashaw JB Jr. Quantification of increased exposure resulting from orbital rim and orbitozygomatic osteotomy via the frontotemporal transsylvian approach. J Neurosurg. 1999; 91:1020–1026. PMID: 10584849.12. Taguchi Y, Tanaka K, Matsuzawa M, Sekino H. A surgical technique to avoid postoperative enophthalmos in the cranioorbital approach. Technical note. J Neurosurg. 1996; 85:514–517. PMID: 8751643.13. Ota N, Tanikawa R, Miyazaki T, et al. Surgical microanatomy of the anterior clinoid process for paraclinoid aneurysm surgery and efficient modification of extradural anterior clinoidectomy. World Neurosurg. 2015; 83:635–643. PMID: 25527880.14. Zabramski JM, Kiriş T, Sankhla SK, Cabiol J, Spetzler RF. Orbitozygomatic craniotomy. Technical note. J Neurosurg. 1998; 89:336–341. PMID: 9688133.15. Kodera T, Arishima H, Yamada S, et al. Orbitozygomatic craniotomy with modified Zabramski's technique: a technical note and anatomic and clinical findings. World Neurosurg. 2017; 97:49–57. PMID: 27693820.16. Mercier P, Brassier G, Fournier HD, Delion M, Papon X, Lasjaunias P. Morphological anatomy of the cranial nerves in their cisternal segment (III-XII). Neurochirurgie. 2009; 55:78–86. PMID: 19328500.17. Son BC, Lee SW, Kim S, Hong JT, Sung JH, Yang SH. Transzygomatic approach with intraoperative neuromonitoring for resection of middle cranial fossa tumors. J Neurol Surg B Skull Base. 2012; 73:28–35. PMID: 23372992.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Modified Transsylvian Approach with Orbitozygomatic Resection for Distal Basilar Artery Aneurysms
- Temporal Approach for Sellar or Parasellar Lesions
- Surgical Tacties for Large Sellar and Parasellar Tumors
- Surgical Results of Anterior Circulation Aneurysm by Inexperienced Neurosurgeon
- Thrombosed Giant Posterior Communicating Aneurysm Simulating Brain Neoplasm: A Case Report
