Transarterial chemoembolization using drug-eluting bead compared with radiofrequency ablation for treatment of single small hepatocellular carcinoma: a pilot non-randomized trial
- Affiliations
-
- 1Department of Internal Medicine, Cheju Halla General Hospital, Jeju, Korea
- 2Department of Internal Medicine, Yonsei University Medical College, Seoul, Korea
- 3Department of Radiology, Cheju Halla General Hospital, Jeju, Korea
- KMID: 2520901
- DOI: http://doi.org/10.17998/jlc.2021.05.20
Abstract
- Background/Aims
Surgical resection, transplantation, and radiofrequency ablation (RFA) are generally accepted as amenable treatments for small hepatocellular carcinoma (HCC). Recently drug-eluting beads (DEB) which had several treatment advantages were introduced for transarterial chemoembolization (TACE). The aim of this study was to evaluate feasibility and safety of DEB-TACE compared with RFA for the treatment of single small HCC.
Methods
In this pilot non-randomized trial, we assessed retrospective data of 40 patients who underwent DEB-TACE (n=21) or RFA (n=19) for single small (≤3 centimeter in greatest dimension) HCC. The primary outcomes were tumor response and time to recurrence. The secondary outcome was treatment-related complications.
Results
Complete response rate to DEB-TACE and RFA after first follow-up assessment was 90.5% and 94.7%, respectively (P=1.000). During mean follow-up of 87.6 months (95% confidence interval: 74.4-102), 7 patients experienced local recurrence. The 6- and 12-month cumulative local recurrence rate was 5.0% and 21.8% in DEB-TACE vs. 11.1% and 17.0% in RFA group (P=0.877). A total 14 distant intrahepatic recurrences were developed and 12- and 24-month cumulative distant intrahepatic recurrence rate was 20.6% and 42.7% in DEBTACE vs. 17.2% and 36.3% in RFA group (P=0.844). Two patients experienced gangrenous cholecystitis after DEB-TACE requiring cholecystectomy as treatment-related adverse event.
Conclusions
Tumor response and recurrence rate after single session of DEB-TACE or RFA were similar. DEB-TACE could be applied selectively in patients with a single small HCC if the other therapeutic modality is unfeasible.
Keyword
Figure
-

Figure 1 Solitary enhancing nodule measuring 2.0 cm in the liver segment 6 was noted on dynamic computed tomography (CT) (A: arterial phase, arrow) and gadoxetic acid-enhanced magnetic resonance imaging (MRI) (B: arterial, C: equillibrium, D: hepatobiliary phases, E: T2-weight, F: diffusion-weighted image) in 75-year-old male patient. Selective right hepatic arteriography demonstrated the faint tumor staining (G, arrow). Post-embolization arteriography (H) showed no more tumor staining and occlusion of the tumor supplying artery. Complete necrosis of the hepatocellular carcinoma nodule without remnant or new enhancement was observed on follow-up CT (I: arterial phase) and MRI (J: arterial phase). There is no local tumor recurrence 28.6 months after a single session of drug-eluting bead transarterial chemoembolization.
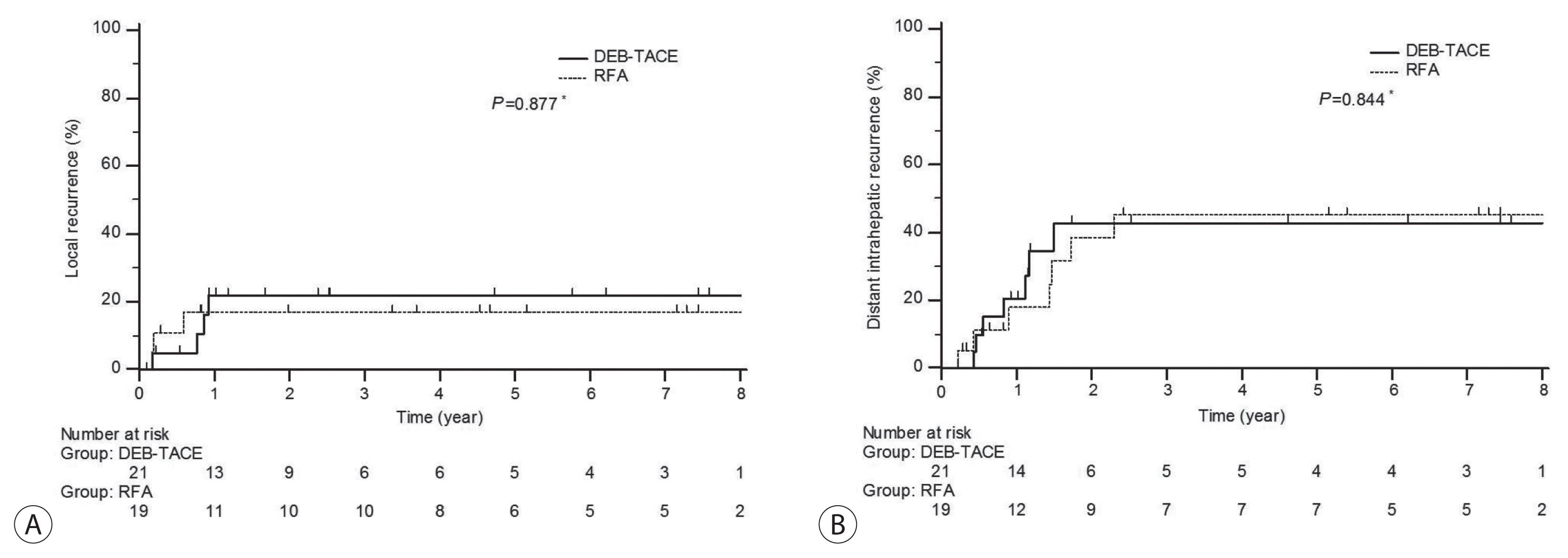
Figure 2 Estimated cumulative recurrence rate after drug-eluting bead transarterial chemoembolization (DEB-TACE) and radiofrequency ablation (RFA) for small hepatocellular carcinoma. Local (A) and distant intrahepatic (B) recurrences. *P-values were calculated using log-rank test for differences between two groups.

Figure 3 A 77-year-old woman who experienced acute cholecystitis requiring cholecystectomy after drug-eluting bead transarterial chemoembolization (DEB-TACE). 1.4 cm sized, typical hypervascular nodule with delayed washout at segment 5 (A, arrow) showed complete necrosis on dynamic computed tomography (CT) (B) that was taken 7 days after DEB-TACE. Acute cholecystitis impending gangrenous change was noted on the same follow-up CT (C). Emergency cholecystectomy was performed 10 days after DEB-TACE in spite of administration of antibiotics with vigorous intravenous hydration. Resected specimen revealed acute ischemic cholecystitis with deposition of embolic particles in the vessel (D, gross specimen; E, original magnification [×40]; F, original magnification [×200]).
Reference
-
References
1. Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol. 2006; 45:529–538.2. Bruix J, Sherman M. Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005; 42:1208–1236.3. Llovet JM, Di Bisceglie AM, Bruix J, Kramer BS, Lencioni R, Zhu AX, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst. 2008; 100:698–711.4. Bruix J, Sala M, Llovet JM. Chemoembolization for hepatocellular carcinoma. Gastroenterology. 2004; 127(5 Suppl 1):S179–S188.5. Lencioni R. Loco-regional treatment of hepatocellular carcinoma. Hepatology. 2010; 52:762–773.6. Hong K, Khwaja A, Liapi E, Torbenson MS, Georgiades CS, Geschwind JF. New intra-arterial drug delivery system for the treatment of liver cancer: preclinical assessment in a rabbit model of liver cancer. Clin Cancer Res. 2006; 12:2563–2567.7. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982; 5:649–655.8. Heimbach JK, Kulik LM, Finn RS, Sirlin CB, Abecassis MM, Roberts LR, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018; 67:358–380.9. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018; 69:182–236.10. Ahn SS, Kim MJ, Lim JS, Hong HS, Chung YE, Choi JY. Added value of gadoxetic acid-enhanced hepatobiliary phase MR imaging in the diagnosis of hepatocellular carcinoma. Radiology. 2010; 255:459–466.11. Doyle A, Gorgen A, Muaddi H, Aravinthan AD, Issachar A, Mironov O, et al. Outcomes of radiofrequency ablation as first-line therapy for hepatocellular carcinoma less than 3 cm in potentially transplantable patients. J Hepatol. 2019; 70:866–873.12. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010; 30:52–60.13. National Cancer Institute. Common terminology criteria for adverse events (CTCAE) version 4.0. 2009. [Internet]. Bethesda (MD): National Cancer Institute;[cited 2020 Nov 14]. Available from: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CT-CAE_4.03_2010-06-14_QuickReference_5x7.pdf .14. Marrero JA, Kulik LM, Sirlin CB, Zhu AX, Finn RS, Abecassis MM, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018; 68:723–750.15. Omata M, Cheng AL, Kokudo N, Kudo M, Lee JM, Jia J, et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatol Int. 2017; 11:317–370.16. Korean Liver Cancer Association; National Cancer Center. 2018 Korean Liver Cancer Association-National Cancer Center Korea practice guidelines for the management of hepatocellular carcinoma. Gut Liver. 2019; 13:227–299.17. Nault JC, Sutter O, Nahon P, Ganne-Carrié N, Séror O. Percutaneous treatment of hepatocellular carcinoma: state of the art and innovations. J Hepatol. 2018; 68:783–797.18. Brunello F, Cantamessa A, Gaia S, Carucci P, Rolle E, Castiglione A, et al. Radiofrequency ablation: technical and clinical long-term outcomes for single hepatocellular carcinoma up to 30 mm. Eur J Gastroenterol Hepatol. 2013; 25:842–849.19. Francica G, Saviano A, De Sio I, De Matthaeis N, Brunello F, Cantamessa A, et al. Long-term effectiveness of radiofrequency ablation for solitary small hepatocellular carcinoma: a retrospective analysis of 363 patients. Dig Liver Dis. 2013; 45:336–341.20. Varela M, Real MI, Burrel M, Forner A, Sala M, Brunet M, et al. Chemoembolization of hepatocellular carcinoma with drug eluting beads: efficacy and doxorubicin pharmacokinetics. J Hepatol. 2007; 46:474–481.21. Poon RT, Tso WK, Pang RW, Ng KK, Woo R, Tai KS, et al. A phase I/II trial of chemoembolization for hepatocellular carcinoma using a novel intra-arterial drug-eluting bead. Clin Gastroenterol Hepatol. 2007; 5:1100–1108.22. Lee KH, Joo SM, Yum TJ, Jung SH. Conventional versus drug-eluting beads trans-arterial chemoembolization for treatment of hepatocellular carcinoma at very early and early stages. J Liver Cancer. 2017; 17:144–152.23. Lammer J, Malagari K, Vogl T, Pilleul F, Denys A, Watkinson A, et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc Intervent Radiol. 2010; 33:41–52.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Drug-Eluting Bead Transarterial Chemoembolization Versus Radiofrequency Ablation as an Initial Treatment of Single Small (≤ 3 cm) Hepatocellular Carcinoma
- The Role of Combination of Transarterial Chemoebolization and Radiofrequency Ablation for Hepatocellular Carcinoma Treatment
- Complications Related to Transarterial Treatment of Hepatocellular Carcinoma: A Comprehensive Review
- Transarterial chemoembolization using drug eluting beads for the treatment of hepatocellular carcinoma: Now and future
- Efficacy of Hepatic Arterial Infusion Chemotherapy and Radiofrequency Ablation against Hepatocellular Carcinoma Refractory to Transarterial Chemoembolization and Vascular Variation: A Case Study
